|
History > 2006 > USA > Health (II)

Dr. Sara Gibson,
in her office in Flagstaff, Ariz.,
meets with
a patient more than 100 miles away in St. Johns.
Jeff Topping for The New York Times
June 7, 2006
TV Screen, Not Couch, Is Required for This
Session
NYT
8.6.2006
http://www.nytimes.com/2006/06/08/us/08teleshrink.html
The New Age
Live Long? Die Young?
Answer Isn’t Just in
Genes
August 31, 2006
The New York Times
By GINA KOLATA
Josephine Tesauro never thought she would live
so long. At 92, she is straight backed, firm jawed and vibrantly healthy, living
alone in an immaculate brick ranch house high on a hill near McKeesport, a
Pittsburgh suburb. She works part time in a hospital gift shop and drives her
1995 white Oldsmobile Cutlass Ciera to meetings of her four bridge groups, to
church and to the grocery store. She has outlived her husband, who died nine
years ago, when he was 84. She has outlived her friends, and she has outlived
three of her six brothers.
Mrs. Tesauro does, however, have a living sister, an identical twin. But she and
her twin are not so identical anymore. Her sister is incontinent, she has had a
hip replacement, and she has a degenerative disorder that destroyed most of her
vision. She also has dementia. “She just does not comprehend,” Mrs. Tesauro
says.
Even researchers who study aging are fascinated by such stories. How could it be
that two people with the same genes, growing up in the same family, living all
their lives in the same place, could age so differently?
The scientific view of what determines a life span or how a person ages has
swung back and forth. First, a couple of decades ago, the emphasis was on
environment, eating right, exercising, getting good medical care. Then the view
switched to genes, the idea that you either inherit the right combination of
genes that will let you eat fatty steaks and smoke cigars and live to be 100 or
you do not. And the notion has stuck, so that these days, many people point to
an ancestor or two who lived a long life and assume they have a genetic gift for
longevity.
But recent studies find that genes may not be so important in determining how
long someone will live and whether a person will get some diseases — except,
perhaps, in some exceptionally long-lived families. That means it is generally
impossible to predict how long a person will live based on how long the person’s
relatives lived.
Life spans, says James W. Vaupel, who directs the Laboratory of Survival and
Longevity at the Max Planck Institute for Demographic Research in Rostock,
Germany, are nothing like a trait like height, which is strongly inherited.
“How tall your parents are compared to the average height explains 80 to 90
percent of how tall you are compared to the average person,” Dr. Vaupel said.
But “only 3 percent of how long you live compared to the average person can be
explained by how long your parents lived.”
“You really learn very little about your own life span from your parents’ life
spans,” Dr. Vaupel said. “That’s what the evidence shows. Even twins, identical
twins, die at different times.” On average, he said, more than 10 years apart.
The likely reason is that life span is determined by such a complex mix of
events that there is no accurate predicting for individuals. The factors include
genetic predispositions, disease, nutrition, a woman’s health during pregnancy,
subtle injuries and accidents and simply chance events, like a randomly
occurring mutation in a gene of a cell that ultimately leads to cancer.
The result is that old people can appear to be struck down for many reasons, or
for what looks like almost no reason at all, just chance. Some may be more
vulnerable than others, and over all, it is clear that the most fragile are
likely to die first. But there are still those among the fragile who somehow
live on and on. And there are seemingly healthy people who die suddenly.
Some diseases, like early onset Alzheimer’s and early onset heart disease, are
more linked to family histories than others, like most cancers and Parkinson’s
disease. But predisposition is not a guarantee that an individual will develop
the disease. Most, in fact, do not get the disease they are predisposed to. And
even getting the disease does not mean a person will die of it.
There are, of course, some valid generalizations. On average, for example, obese
men who smoke will die sooner than women who are thin and active and never get
near a cigarette. But for individuals, there is no telling who will get what
when or who will succumb quickly and who will linger.
“We are pretty good at predicting on a group level,” said Dr. Kaare Christensen,
a professor of epidemiology at the University of Southern Denmark. “But we are
really bad on the individual level.”
Looking to Twins
James Lyons used to think his life would be short. Mr. Lyons, a retired
executive with the Boy Scouts of America, thought of his father, who died at 55.
“He had one heart attack. It was six hours from onset to death, and that was
it.”
Then there were his first cousins on his father’s side. One died at 57 and
another at 50. “He was in a barber chair and had a heart attack,” Mr. Lyons said
of the 50-year-old. “He died on the spot.”
“He was a big strapping guy, 6-4, healthy and energetic. Then, boom. One day he
was there, and the next day he was gone.”
“I approached my 50’s with trepidation,” said Mr. Lyons, who lives in Lansing,
Mich.
But his 50’s came and went, and now he is 75. He is still healthy, and he has
lived longer than most of his ancestors. He is baffled as to why.
It seems like common sense. Family members tend to look alike. And many
characteristics are strongly inherited — height, weight, a tendency to develop
early onset heart disease or to get diabetes. Even personalities run in
families. Life span would seem to fit with the rest.
But scientists have been trying for decades to find out if there really is a
strong genetic link to life spans and, if so, to what extent.
They turned to studies of families and of parents and children, but data
analysis has been difficult and any definitive answer elusive. If a family’s
members tend to live to ripe old ages, is that because they share some genes or
because they share an environment?
“Is it good socioeconomic status, good health or good genes?” Dr. Christensen
asked. “How can you disentangle it?”
His solution, a classic one in science, was to study twins. The idea was to
compare identical twins, who share all their genes, with fraternal twins, who
share some of them. To do this, Dr. Christensen and his colleagues took
advantage of detailed registries that included all the twins in Denmark, Finland
and Switzerland born from 1870 to 1910. That study followed the twins until 2004
to 2005, when nearly all had died.
Now, Dr. Christensen and his colleagues have analyzed the data. They restricted
themselves to twins of the same sex, which obviated the problem that women tend
to live longer than men. That left them with 10,251 pairs of same-sex twins,
identical or fraternal. And that was enough for meaningful analyses even at the
highest ages. “We were able to disentangle the genetic component,” Dr.
Christensen said.
But the genetic influence was much smaller than most people, even most
scientists, had assumed. The researchers reported their findings in a recent
paper published in Human Genetics. Identical twins were slightly closer in age
when they died than were fraternal twins.
But, Dr. Christensen said, even with identical twins, “the vast majority die
years apart.”
The investigators also asked when the genetic factor kicked in. One hypothesis,
favored by Dr. Christensen, was that the strongest genetic effect was on deaths
early in life. He thought that deaths at young ages would reflect things like
inherited predispositions to premature heart disease or to fatal cancers.
But there was almost no genetic influence on age of death before 60, suggesting
that early death has a large random component — an auto accident, a fall. In
fact, the studies of twins found almost no genetic influence on age of death
even at older ages, except among people who live to be very old, the late 80’s,
the 90’s or even 100. The average age at which people are dying today in the
United States is 68.5 for men, and 76.1 for women, according to Arialdi M. Minio
of the National Center for Health Statistics. This statistic differs from life
expectancy, which estimates how long people born today are expected to live.
Finding Randomness
Even though there may be a tendency in some rare families to live
extraordinarily long, the genetic influence that emerged from the studies of
twins was significantly less than much of the public and many scientists think
it is.
A woman whose sister lived to be 100 has a 4 percent chance of living that long,
Dr. Christensen says. That is better than the 1 percent chance for women in
general, but still not very great because the absolute numbers, 1 out of 100 or
4 out of 100, are still so small. For men, the odds are much lower. A man whose
sister lived to be 100 has just a 0.4 percent chance of living that long. In
comparison, men in general have a 0.1 percent chance of reaching 100.
Those data fit well with animal studies, says Caleb Finch, a researcher on aging
at the University of Southern California. Genetically identical animals — from
worms to flies to mice — living in the same environments die at different times.
The reason is not known, Dr. Finch said.
“It’s random,” he said. “Since we can’t find any regular pattern, that’s the
hand wave explanation — randomness.”
And random can mean more than one thing.
“There are two phases of randomness,” Dr. Finch said. “There’s the randomness of
life experiences. The unlucky ones, who get an infection, get hit on the head or
get mutations that turn a cell into cancer. And there are random events in
development.”
Random cell growth and division and random differences in which genes get turned
on and how active they are during development can cause identical twins to have
different numbers of cells in their kidneys and even different patterns of folds
in their brains, Dr. Finch pointed out. And random differences in development
early in life can set the stage for deterioration decades later.
But seemingly random events can still come as a shock. That’s how Annmarie Bald
felt when her identical twin, Catherine Polk, died in her sleep of a heart
attack. It happened seven years ago, when Ms. Polk was 43. To this day, Ms.
Bald, of Forked River, N.J., lives in fear that the same thing will happen to
her. She nervously sees her doctor every year for a checkup, and every year her
doctor tells her the same thing: her heart is fine.
“The question in my mind every day is, ‘How did I end up still here and she’s
gone?’ ” Ms. Bald said. “It’s not something you ever get over.”
Yet even diseases commonly thought to be strongly inherited, like many cancers,
are not, researchers found. In a paper in The New England Journal of Medicine in
2000, Dr. Paul Lichtenstein of the Karolinska Institute in Stockholm and his
colleagues analyzed cancer rates in 44,788 pairs of Nordic twins. They found
that only a few cancers — breast, prostate and colorectal — had a noticeable
genetic component. And it was not much. If one identical twin got one of those
cancers, the chance that the other twin would get it was generally less than 15
percent, about five times the risk for the average person but not a very big
risk over all.
Looked at one way, the data say that genes can determine cancer risk. But viewed
another way, the data say that the risk for an identical twin of a cancer
patient is not even close to 100 percent, as it would be if genes completely
determined who would get the disease.
Dr. Robert Hoover of the National Cancer Institute wrote in an accompanying
editorial: “There is a low absolute probability that a cancer will develop in a
person whose identical twin — a person with an identical genome and many similar
exposures — has the same type of cancer. This should also be instructive to some
scientists and others interested in individual risk assessment who believe that
with enough information, it will be possible to predict accurately who will
contract a disease and who will not.”
Alzheimer’s disease also has a genetic component, but genes are far from the
only factor in determining who gets the disease, said Margaret Gatz of the
University of Southern California and Nancy Pedersen of the Karolinska
Institute.
Dr. Gatz and Dr. Pedersen analyzed data from a study of identical and fraternal
Swedish twins 65 and older. If one of a pair of identical twins developed
Alzheimer’s disease, the other had a 60 percent chance of getting it. If one of
a pair of fraternal twins, who are related like other brothers and sisters, got
Alzheimer’s, the other had a 30 percent chance of getting it.
But, Dr. Pedersen noted, Alzheimer’s is so common in the elderly that it occurs
in 35 percent of people age 80 and older. If genes determine who gets
Alzheimer’s at older ages, Dr. Pedersen says, “those genes must be very common,
have small effects and probably interact with the environment.”
As for other chronic diseases of the elderly, Parkinson’s has no detectable
heritable component, studies repeatedly find. Heart disease appears to be
indiscriminate, striking almost everyone eventually, says Dr. Anne Newman of the
University of Pittsburgh, who has studied it systematically in a large group of
elderly people.
But the general picture is consistent in study after study. A strong family
history of even a genetically linked disease does not guarantee a person will
get it, and having no family history does not mean a person is protected.
Instead, chronic diseases strike almost at random among the elderly, making it
perhaps not so surprising that life spans themselves have such a weak genetic
link.
Matt McGue, a psychology professor at the University of Minnesota who studies
twins, contrasts life spans with personality, which, he says, is about 50
percent heritable, or attention-deficit hyperactivity disorder, which is 70 to
80 percent heritable, or body weight, which is 70 percent heritable.
“I’ve been in this business for a long while, and life span is probably one of
the most weakly heritable traits I’ve ever studied,” Dr. McGue said.
Seeking Rare Families
At the National Institute on Aging, the question still hovers: Is it possible to
find genetic determinants of exceptional health and longevity?
“If you could identify factors for exceptionally good health, that might allow
people to avoid disease,” said Evan Hadley, director of the institute’s
geriatrics and clinical gerontology program.
There are two methods to do this, Dr. Hadley said. One is to look at how the
genes of centenarians differ from those of the rest of the population. But, he
said, that requires that if longevity genes exist, they are common among
centenarians. And, so far, such studies have not yielded much that has held up —
with one well accepted exception: a gene for a cholesterol-carrying protein that
affects risk for heart disease as well as Alzheimer’s disease. Those who have
that gene have double the chances of living to 100. But that chance is not much
anyway. Only about 2 percent of people born in 1910 could expect to reach 100.
The second approach is to look for rare genes in unusually long-lived families.
“If there is something in a family, it may be in only one or a few families,”
Dr. Hadley said. But it may have a big effect.
So the National Institute on Aging is starting a research project with
investigators at three United States medical centers and at Dr. Christensen’s
center in Denmark. The plan is to find exceptional families, those in which
there is a cluster of very old, closely related members — two sisters in their
90’s, for example — whose children, who would typically be in their 70’s, and
grandchildren, can be studied too.
Today, many families have a few members living to advanced ages, but very few
families have many of them. And in large families, just by chance, someone may
live past 90, but it is unlikely that most of the brothers and sisters will get
there. For these families, there does not appear to be a genetic component to
life spans.
For now, the study is in a pilot phase, testing a scoring system to define the
families who seem to fit the criteria.
“If you are really, really old in a family, that gets you more points,” Dr.
Hadley said. “You get more points for being 97 than for being 92. But we also
are looking at the whole family structure. If there are just two siblings in a
family and both live to 98, that’s very exceptional. But suppose there are eight
kids and they all made it to 87. That’s pretty unusual, too.’’
If the researchers find genes in the oldest family members that seem to be
associated with protection from a disease like heart disease and with a long
life, they will follow the younger members of the family, children in their 60’s
and 70’s, asking if the same genes seem to protect them as they age.
Some wonder if the project can succeed, said Dr. Newman, who is directing one
study center, at the University of Pittsburgh. “The big debate is, is it
possible for there to be a few genes that are protective or is it going to be so
complicated that we won’t be able to figure out the genetic factors? Is it going
to be that some people are just lucky?”
She is optimistic, reasoning that since some families tend to have early onset
of certain diseases, others probably have a genetic predisposition to get
diseases like heart disease, cancer and Alzheimer’s so late that most members do
not get them at all and live very long and healthy lives.
“This would be the flip side of early onset,” she says.
Mrs. Tesauro is in the pilot study. She had always been healthy and active, a
self-described tomboy growing up who played tennis until she was 85. “I just
can’t sit still,” she said.
She was a woman who knew her mind, so eager to go to college that she defied her
father, who thought it was a waste of money, and worked her way through. She
ended up with a master’s degree in education and a career as a high school
teacher.
Her twin was different. She was the frilly type, Mrs. Tesauro said, and was not
much of a student. She failed a grade in high school and barely graduated. Both
Mrs. Tesauro and her sister married and had children.
Mrs. Tesauro was born first, and it is a common belief even among scientists
that the twin born first is stronger and lives longer. But when he looked at the
Scandinavian data, Dr. Christensen said, he found that birth order made no
difference in health or longevity.
The day before visiting Mrs. Tesauro for the first time, the Pittsburgh
investigators tried to call her, just to be sure she was still alive and still
healthy enough to be interviewed. When they could not reach her, they began to
worry.
But all was well. Mrs. Tesauro answered the phone the next morning and explained
why they had had such trouble. She was out running errands.
Live
Long? Die Young? Answer Isn’t Just in Genes, NYT, 31.8.2006,
http://www.nytimes.com/2006/08/31/health/31age.html
Clinton Makes Up
for Lost Time in Battling
AIDS
August 29, 2006
The New York Times
By CELIA W. DUGGER
RWINKWAVU, Rwanda — Bill Clinton worked the
crowd of AIDS survivors, clasping the outstretched hands of children alive
because of the AIDS medicines his foundation donated.
Inside the rural hospital here that he recently helped renovate, where Rwandans
were hunted down and killed during the genocide he regrets he didn’t try to stop
as president, Mr. Clinton heard people once skeletal from AIDS tell of their
resurrections to robust health.
Since he left office more than five years ago at age 54, one of the youngest
former presidents ever, Mr. Clinton has made a lasting mark in a cause that he
came to only late in his presidency: fighting the AIDS pandemic across Africa
and the world.
Few public figures in America have spawned as much speculation about what
motivates them as Mr. Clinton. Abroad, even fewer inspire the affectionate
reception Mr. Clinton received as he raced across seven African countries in
eight days in July. Crowds at roadsides and in hospitals wanted to touch him —
and he obliged by shaking hands, kissing babies and hugging people with AIDS.
Here on Mr. Clinton’s fourth visit to Rwanda, it was clear the efforts by his
foundation had personal meaning. He said he was sorry his administration failed
to intervene during the 1994 genocide. “The United States just blew it in
Rwanda,” he said flatly. Paul Kagame, Rwanda’s president, said he had accepted
Mr. Clinton’s repeated apologies.
But on this trip, Mr. Clinton seemed anything but a man tormented by guilt.
Rather, he reveled in his role as a private citizen championing people with
AIDS.
“The reason I do this work I do is that I really care about politics and people
and public policy,” he said in one of several interviews, scornfully dismissing
questions about whether his global AIDS work is a form of redemption for what he
failed to accomplish on the issue as president, or for the Monica Lewinsky
scandal. “I’m 60 years old now, and I’m not running for anything, so I don’t
have to be polite anymore,” he said. “I think it’s all a bunch of hokum,” he
added, calling such speculation psychobabble.
“I have never met anybody who spent all their time talking about everybody’s
motives who at the end of their life could talk about very many lives they had
saved,” he said.
Mr. Clinton was adamant that he had done all he could about global AIDS with a
Congress hostile to foreign aid, though he conceded that his administration
fought too long to protect the patent rights of pharmaceutical companies against
countries trying to make or import cheaper AIDS medicines.
‘Everyone Was Worried’
After he left office, Mr. Clinton faced some skepticism as he took up the cause
of people with AIDS dying faraway deaths in poor countries. His administration,
which sought more resources to combat AIDS domestically, had a far weaker claim
to leadership on AIDS worldwide.
When doctors specializing in public health met him at the William J. Clinton
Foundation in Harlem in the fall of 2002, Howard Hiatt, the former dean of the
Harvard School of Public Health, bluntly asked Mr. Clinton why those present
should expect that “you’ll be able to accomplish now what you didn’t undertake
in your presidency — an attack on this plague?”
“Everyone was worried,” said Richard Marlink, who headed Harvard’s AIDS
Institute. “Is this a campaign with photo ops and press releases or a long-term
commitment?”
In the years since, doctors at the forefront of AIDS treatment have worked with
Mr. Clinton. Dr. Marlink volunteered to help Mr. Clinton’s foundation in South
Africa. Dr. Hiatt, who serves on the board of Partners in Health, a nonprofit
group that works with Mr. Clinton in Rwanda, said the former president “has
really perceived the seriousness of the problem.”
Mr. Clinton and his foundation have undertaken projects with two dozen
developing countries, raising money to post nurses in rural clinics in Kenya,
mustering experts to train hospital managers in Ethiopia and buying drugs for
thousands of sick children, among other things.
His foundation also has negotiated steep cuts in the price of AIDS medicines
through deals with drug companies that cover more than 400,000 patients in
dozens of countries, helping propel momentum for treatment of the destitute.
Dr. Bernard Pécoul, who led a campaign for access to medicines for Doctors
Without Borders from 1998 to 2003, credited Mr. Clinton and his foundation for
showing independence from the politically powerful drug industry and helping to
accelerate the decline in prices for generic AIDS medicines in developing
countries.
“They have been very clever in supporting generic policy in the United States, a
country where it’s not easy,” he said. “And sometimes they’ve been even more
courageous than the United Nations system, which is under pressure from member
states.”
The Clinton foundation’s budget last year was $30 million, raised from private
donors. Mr. Clinton, who oversees its operations full time, has plunged into
many causes, from childhood obesity to tsunami relief to global warming, but he
has made his most substantive contribution on AIDS.
He said Rwanda was one of the first countries he chose to work in because “they
had a really good chance to dig out of the hole and I wanted to help them do
it.”
For years, he tried to coax Dr. Paul Farmer, known for his work caring for the
poor in remote, rural Haiti, to recreate his model of AIDS treatment in Africa,
the heart of the epidemic.
Last year, Dr. Farmer and the group he co-founded, Partners in Health, arrived
in Rwinkwavu. With support from the Clinton Foundation and others, he has
transformed a dilapidated facility that lacked even a doctor into a thriving
rural hospital.
More than 1,500 people have been put on AIDS medicines here. Reproducing the
pioneering model used in Haiti, Dr. Farmer has community workers, many of them
peasants, deliver antiretroviral medicines to people with AIDS every day,
minimizing reliance on scarce doctors and nurses.
Like most international leaders and American advocates for people with AIDS in
the 1990’s, critics say, Mr. Clinton’s efforts on global AIDS did not match the
epic scale of the human tragedy as it unfolded across Africa and millions died
and were orphaned.
In recent years, the fight against AIDS has leapt onto the world stage, claimed
by Mr. Clinton and his Republican successor, George W. Bush.
There is a measure of irony in this. Since 2003, Mr. Bush has marshaled billions
of dollars in American assistance for a global assault on the disease, financing
lifesaving treatment for hundreds of thousands of people with AIDS. Yet because
of his foreign policies, notably the war in Iraq, he is often met by protests
when he travels abroad, while Mr. Clinton is warmly embraced across the
developing world.
“George Bush has actually delivered more resources, but Clinton is ten times
more popular in Africa,” said Princeton Lyman, who was American ambassador to
South Africa under Mr. Clinton. “That’s because, just like he does everywhere,
he portrays that sense that he cares.”
On his recent tour of Africa — his fifth since 2001 — Mr. Clinton showed a
remarkable ability to establish a human connection with people he met.
In Johannesburg, Mr. Clinton and a frail Nelson Mandela, about to turn 88,
clutched each other’s hands like a long-lost son and his beloved father.
En route to the airport in Lilongwe, Malawi, where crowds of people strained to
catch a glimpse of him, Mr. Clinton suddenly halted the motorcade, conducted an
impromptu interview in the middle of the road, then plunged into a throng of
young men reaching out to touch him.
At a hospital in Mafeteng, Lesotho, Mr. Clinton strolled into a sunny courtyard
with 6-year-old Arriet Moeketsi, a little girl in a polka-dot dress. Arriet, who
takes AIDS medicines donated by Mr. Clinton’s foundation, trustingly leaned her
face against the former president and never let go of his hands during a
prolonged news conference.
Bill and Melinda Gates, the billionaire philanthropists, watched. Mr. Clinton
had visited an AIDS project of theirs in Durban, South Africa, and they had come
to Lesotho to see his work. When Mr. Clinton left the hospital with Arriet, a
Clinton volunteer asked the Gateses to stay back so photographers could follow
him.
The world’s wealthiest couple seemed to take no offense. The two Bills, as they
have been dubbed, have taken to doing high-profile AIDS advocacy events
together, with Mr. Clinton bringing star power and Mr. Gates his deep pockets.
“He plays a unique role in shining a light on the problem,” said Mr. Gates,
after he made it into the courtyard.
Mr. Clinton has come a long way on global AIDS. For most of his presidency, his
trade office fought to protect the patent rights of pharmaceutical companies
against attempts by developing countries to make or import cheaper generic
medicines. “I think it was wrong,” he now says of that approach.
During the first six years of his presidency, federal spending to fight AIDS
worldwide stagnated at paltry levels, never topping $141 million.
But by his last budget, spending more than tripled to $540 million, but Mr.
Clinton says that was far from enough. Even so, he contends that no one could
have done better.
The Role of Congress
The Democrats controlled Congress for only his first two years in office, he
pointed out, when “everybody’s obsession” was the AIDS problem in America. After
that, the Republican-dominated Congress that later supported Mr. Bush’s $15
billion, five-year global AIDS plan fiercely resisted spending on foreign
assistance.
“Have you forgotten what I had in the Congress?” he asked. “That the Republican
Congress spent all their time trying to trash me?
“And the only reason they gave money to George Bush for AIDS is they wanted to
have something they looked progressive on since they were cutting taxes for rich
people like me,” he said.
Michael Gerson, who was a senior adviser to Mr. Bush on global health issues,
noted that the Republican Congress was, in fact, open to persuasion that global
AIDS was a spending priority. But he also said the issue had ripened by the time
Mr. Bush was president. The price of antiretroviral drugs fell after Mr. Clinton
left office, helping change the view that it was too costly and difficult to
treat people in poor countries.
But Mr. Gerson also said of the Clinton record: “I don’t believe they were
visionary or pushed the system. I don’t think they were thinking big.”
The debate over whether Mr. Clinton missed a political opportunity to lead the
charge on global AIDS years before Mr. Bush seized it is far from over.
Greg Behrman, the author of “The Invisible People: How the U.S. Has Slept
Through the Global AIDS Pandemic, the Greatest Humanitarian Catastrophe of Our
Time,” offers a split verdict.
“There are two acts here,” he said. “Clinton’s post-presidential leadership has
been extraordinary. As president, though, the record is clear. Clinton was not a
leader on global AIDS and the consequences have been devastating.”
After he left office, Mr. Clinton considered his future with a keen eye on
history, analyzing what former presidents had done.
He concluded that another former Southern governor, Jimmy Carter, a Nobel Peace
Prize winner who is now recognized for his work on human rights, democracy and
neglected diseases, was “the only person who’d done anything that remotely
resembled what I thought I could do.”
From the start, Mr. Clinton had a host of issues on his agenda, but quickly
found himself drawn into AIDS. He turned to his old friend Ira Magaziner, a
fellow Rhodes scholar and corporate consultant who had managed the Clintons’
failed health care reform effort. Mr. Magaziner has since led the foundation’s
AIDS program.
The two men discovered in 2002 that the Bahamas was paying $3,500 per person a
year for generic AIDS drugs. “I said, ‘Ira, please find out why in the hell
these people are paying $3,500 for $500 drugs,’ ” Mr. Clinton said.
They learned the Bahamas was buying through middlemen, so the foundation helped
the country purchase directly from Cipla, the Indian generic-drug manufacturer.
“So our first victory was a lay-down,” Mr. Clinton said. “All of a sudden, they
could treat six times as many people for the same amount of money.”
Opportunities proliferated, and Mr. Clinton’s enthusiasm grew.
His name opened doors with generic drug makers. With growing demand for AIDS
drugs already on the horizon, as well as the economies of scale that come with
that, Mr. Magaziner took a team of volunteer consultants to India in 2003 to
negotiate for lower prices. Companies opened their books.
“The name Clinton in India holds more charisma and credibility than any other
American name,” said Dr. Yusuf K. Hamied, Cipla’s chairman.
Through cost cutting, spurred by breakthrough talks with companies that supplied
ingredients to the drug makers, the team got deals. Cipla, for example, halved
the price of the most common AIDS triple-drug therapy, already declining due to
competition, to $140 a person per year.
Similarly, Mr. Clinton was able to use his relationships with political leaders,
like President Thabo Mbeki of South Africa, who had questioned whether H.I.V.
caused AIDS. The country had not begun treating its people for the disease,
though almost five million had been infected. “He was getting killed in the
global press about it,” Mr. Clinton recalled.
Mr. Clinton, who knew him from his own time as president, met with Mr. Mbeki in
2003 as one politician to another. “I said, ‘You know, I really want to help
you, and as you know, I may be the only one of those involved in this work who’s
never been publicly critical of you,’ ” Mr. Clinton said he told Mr. Mbeki. “
‘But this is something you have to do.’ ”
Mr. Mbeki soon invited Mr. Clinton’s foundation to help the country write a
comprehensive treatment plan. South Africa now has more than 130,000 people on
antiretroviral drugs, still far short of what critics say is needed.
Since 2004, Mr. Clinton has campaigned to raise the profile of children with
AIDS. A scant 20,000 children in the developing world were then getting drug
treatment, while more than 500,000 a year were dying. The Clinton foundation has
raised $4.4 million to buy drugs for 13,000 children, train health workers,
renovate pediatric wings and pay for lab tests.
“Children are alive in numbers we couldn’t have imagined a couple of years ago
because of what he’s done,” said Peter McDermott, chief of H.I.V. and AIDS
programs at Unicef.
Mr. Clinton’s ambitions seem to grow daily, and his foundation is now branching
out in Africa from AIDS into poverty. As he relaxed one recent evening in a
sumptuous, $2,260-a-night suite in Johannesburg, with zebra skin rugs underfoot
(the lodgings provided to him gratis by a rich South African businessman who
owned the hotel), he got excited just thinking about fertilizer.
Mr. Magaziner has people riding trains and trucks that carry fertilizer to
figure out why a commodity that should enable farmers to grow more food and
avoid hunger costs so much in Africa.
“You follow the trail!” Mr. Clinton said.
Mr. Clinton was joined on his trip by Sir Tom Hunter, a Scottish entrepreneur
who has promised to spend $100 million of his fortune in collaboration with the
foundation, much of it on economic development.
“Tom, where’s Tom?” Mr. Clinton called out excitedly as he chatted with
representatives of a nonprofit group that promotes solar-powered lights during
an event here in Rwinkwavu.
What if Rwanda could manufacture such lights locally? Mr. Clinton mused. Why not
electrify villages so children can study at night? “It might be possible to get
a factory here that would serve all of central Africa!”
Clinton Makes Up for Lost Time in Battling AIDS, NYT, 29.8.2006,
http://www.nytimes.com/2006/08/29/health/29clinton.html
Philadelphia yanks HIV ads
showing black
men in gun's cross hairs
Posted 8/8/2006 4:44 PM ET
AP
USA Today
PHILADELPHIA (AP) — Health officials yanked
public service advertisements urging HIV testing after a gay advocacy group
expressed concerns about images depicting young black men in a gun's cross
hairs.
"Putting the face of a black man in the cross
hairs of a gun paints a damaging message about violence and black men," Lee
Carson, chairman of the Black Gay Men's Leadership Council, wrote in a letter to
the city's interim health commissioner last month.
The $236,000 campaign, which ended abruptly Monday, was geared at gay and
bisexual men and featured the tagline, "Have YOU been hit?"
"Given the violence perpetrated against gay men, it is not farfetched to see how
this campaign fosters violence," Carson wrote to interim Health Commissioner
Carmen Paris.
Paris said she "inherited" the campaign and only recently saw the ads. She
added, "The right thing to do, of course, is not to promote any message that
could be perceived as promoting violence."
The campaign was launched May 19 with ads on buses, television, postcards and a
website. The ads were no longer posted on the website Tuesday.
Zigzag Net Inc., the Philadelphia-based marketing company that developed the
campaign, spent months setting up two focus groups to evaluate the most
effective themes.
"We are aware of objections to the campaign," project manager Aaron McLean said.
"However, we acted under the explicit direction of the city Health Department.
The response in the focus groups was very positive."
Philadelphia yanks HIV ads showing black men in gun's cross hairs, UT, 8.8.2006,
http://www.usatoday.com/news/health/2006-08-08-hivads_x.htm
Doctors: Separation of Twins Going Well
August 8, 2006
By THE ASSOCIATED PRESS
Filed at 2:22 a.m. ET
The New York Times
SALT LAKE CITY (AP) -- Doctors have
successfully separated 4-year-old twin sisters born fused at the midsection,
with just one kidney and one set of legs, and were continuing with
reconstruction surgery.
The parents broke into tears when doctors announced that the separation had been
completed at 10:50 p.m., and, at 11 p.m., one -- Kendra Herrin -- was moved to a
separate operating room.
''It's just a new beginning -- and the end of a really good one,'' father Jake
Herrin said.
Reconstruction was expected to take another 4 1/2 hours.
Doctors at Primary Children's Hospital said it was the first known surgical
attempt to separate twins with a shared kidney.
Kendra and Maliyah Herrin were rolled into the operating room at 7:15 a.m. after
a tearful goodbye from their parents.
''It was very emotional,'' said their father, Jake Herrin. ''They were more
brave than us.''
The operation was expected to last 12 to 24 hours, during which surgeons planned
to give each girl one leg and Kendra the kidney. Maliyah will be put on dialysis
for three to six months until she is strong enough for a transplant of a kidney
from her mother, Erin Herrin.
Surgeons also divided the girls' single liver and separated their intestines.
The twins were stable through the first 12 hours of the operation, the doctors
said earlier.
''Going great, no problems whatsoever,'' said Dr. Rebecka Meyers, the hospital's
chief of pediatric surgery. She said the procedures surgeons performed on the
twins are commonly done in many patients -- just not those who are attached to
each other.
''What's unusual is doing them all in one single surgery, in two separate girls,
followed by the physical separation of the children,'' hospital spokeswoman
Bonnie Midget said.
The surgery included successfully separating the intestines, divided and
reconstructed the twins' two bladders.
Surrounded by family and close friends, the girls' parents were being updated
hourly by the surgical team's lead nurse and tried to stay upbeat.
''We know going into this surgery that angels are watching over our children, we
feel it,'' Erin Herrin said.
Jake Herrin said they were grateful for messages posted on the North Salt Lake
family's Web site from well-wishers around the world.
The blue-eyed, sandy-haired girls were born locked in an embrace, practically
face to face. Conjoined twins occur about once in every 50,000 to 100,000
births. Only about 20 percent survive to become viable candidates for
separation.
Monday's surgical team included six surgeons, two anesthesiologists, one
radiologist, two urologists and 25 to 30 support staff members.
------
On the Net:
www.Herrintwins.com
Doctors: Separation of Twins Going Well, NYT, 8.8.2006,
http://www.nytimes.com/aponline/us/AP-Conjoined-Twins.html
Aging face of HIV poses new challenges
Updated 8/4/2006 9:35 PM ET
AP
USA Today
NEW YORK (AP) — Pat Shelton has had the AIDS
virus for at least 15 years, and also struggles with hepatitis C and high blood
pressure. But what is bothering her most on this sultry summer day are hot
flashes.
"I've gone through hell with my menopause,"
said Shelton, an elegant woman who recently swapped her dreadlocks for a
close-cropped look while trying to stay cool. "It's kicking me. But HIV, I've
been very blessed. I don't know why."
The 53-year-old Shelton, whose drug regimen has kept her HIV from developing
into full-blown AIDS, in many ways represents the changing face of the HIV
population in New York and around the country: They are getting older and
presenting new challenges to health care providers.
In New York City, the epicenter of AIDS in the United States, 30% of the 100,000
people with HIV are over 50, and 70% are over 40, according to the city health
department. Nationwide, 27% of people with AIDS are now over 50, the Centers for
Disease Control reported.
"Here is a group of people who, yes, they have HIV, but they're going to get
other illnesses," said Stephen Karpiak, the associate director of research for
the AIDS Community Research Initiative of America (ACRIA). "And we don't know
the interaction of all the drugs. There are God knows how many hundreds of drugs
used by folks for cardiac issues, osteoporosis, arthritis — we don't know those
interactions at all.
"No one's ever looked at them. Someone needs to do trials."
Karpiak's agency conducted a study, released this week, that examined the many
challenges faced by people with the AIDS virus.
The AIDS service organizations that arose after the epidemic hit in the 1980s
were designed to provide care and counseling to people facing shortened life
spans. While there's still no cure for AIDS, anti-retroviral drugs have made it
a manageable illness for many patients and prolonged their lives beyond what
once seemed possible.
As this group ages, they fall prey to a host of conditions that require
medicines that may interfere with the effectiveness of AIDS drugs.
And that's if the condition gets diagnosed at all. AIDS patients typically see
infectious disease specialists who may not have their antennae out for unrelated
diseases, Karpiak said.
They don't look for age-related problems, he said. "That is not their
profession."
Conversely, doctors unfamiliar with AIDS may not suspect that older patients
have the disease.
Because AIDS arose in the United States among gay men, a stigmatized group, it
remains more ostracized than other diseases. Fearing rejection, people with AIDS
often isolate themselves. Isolation becomes more of a problem with age, said
Karpiak, who noted that 70% of the people in the study live alone.
"This is an isolated, stigmatized group of people who have been largely
neglected by their churches, by their communities," he said. "Half have not told
their families. ... And as you age, you need those people for emotional and
everyday support."
Without friends and family, Karpiak said, older people with HIV turn to home
health aides. That creates the potential of overburdening the system as the
number of HIV positive people over 50 continues to rise.
Marjorie Hill of Gay Men's Health Crisis, one of the nation's largest AIDS
service organizations, said 33% of the agency's 15,000 clients are over 50 — up
from 25% two or three years ago.
Among the organization's tailored services are meals and exercise classes better
suited for older clients.
In addition, Hill said, a public service campaign featuring older people —
unlike the subway and magazine ads that typically show images of handsome young
men — is in the works.
"We are actively fundraising to develop a campaign targeting persons over 50
with prevention and education," she said.
Shelton, a former drug user who tested positive for HIV in 1991, has been an
AIDS peer educator since 1998. She is trained to give support but gets support
herself at Copacetic Women, a group for women with HIV over 50.
"I really don't feel too comfortable sitting in a group with people my
children's age," she said. "They're not really going to open up or listen to
what I really have to say. ... We have concerns and health problems that the
doctors are not taking care of. We needed a safe haven."
On the Net: http://www.acria.org
Aging
face of HIV poses new challenges, UT, 4.8.2006,
http://www.usatoday.com/news/health/2006-08-04-aids-aging_x.htm
Kerry Proposes Universal Coverage by 2012
July 31, 2006
By THE ASSOCIATED PRESS
Filed at 1:51 p.m. ET
The New York Times
BOSTON (AP) -- Sen. John Kerry on Monday
proposed requiring all Americans to have health insurance by 2012, ''with the
federal government guaranteeing that they have the means to afford it.''
The Massachusetts Democrat, whose name is figuring prominently in 2008 White
House speculation, repeated his 2004 presidential campaign call for expanding
the federal Medicaid program to cover children. He also proposed creating a
program to cover catastrophic cases so an employer providing insurance doesn't
have to pass the cost to his other workers, and; offering Americans the ability
to buy into the same insurance program used by federal workers such as members
of Congress.
Kerry proposes to pay for the program by repealing tax cuts enacted during the
Bush administration that benefit those earning over $200,000 annually. He did
not immediately elaborate on how he would enact his insurance mandate, but one
aid said he would do so with a requirement written into the legislation spelling
out that the government covers anyone who is uninsured.
''One of my biggest regrets is that fear talk trumped the health care walk, and
that we are less safe abroad and less healthy at home because of that,'' Kerry
told a crowd of several hundred during a midday speech at Faneuil Hall. The
senator had previously delivered two other speeches at the Revolutionary War
meeting house laying the ground work for a second presidential campaign.
The senator also promoted his health care proposal in a Boston Globe op-ed piece
published Monday morning, and during an appearance on Don Imus's national radio
program.
Kerry conceded his health care proposal is virtually the same as the program he
outlined during his failed campaign. However, he said that continuity was a
measure of his commitment to his health care ideals.
''Every day since the election, the health care crisis has grown steadily
worse,'' Kerry said. ''The president has stuck to his guns -- or, more
accurately, his empty holster -- and done nothing beyond trotting out the
conservative hobby horse of health savings accounts.''
The senator said his plan will lead to universal coverage by 2012, ''but if
we're not there by 2012, we will require that all Americans have health
insurance, with the federal government guaranteeing they have the means to
afford it.''
The Republican National Committee, which typically responds to political
criticism of the president, said Kerry's critique ignored the prescription drug
program enacted by the Bush administration.
''It's unfortunate that John Kerry's bitterness over losing the election clouds
his ability to recognize the president's prescription drug plan is providing
millions of seniors with more affordable medicine,'' said RNC spokeswoman Tracey
Schmitt.
Whatever his criticism, Kerry faces the reality that the governor of his home
state -- Republican Mitt Romney, himself a potential 2008 presidential candidate
-- has not only talked about but enacted a sweeping health care overhaul
designed to bring universal coverage to Massachusetts. Last week, Michael
Leavitt, secretary of the U.S. Department of Health and Human services, called
the program ''a model'' for the nation.
Romney negotiated the plan with a Democratic Legislature, and in cooperation
with Sen. Edward M. Kennedy, D-Mass., Kerry's senior colleague.
Under Romney's plan, which the federal government is assisting with $385 million
annually, Medicaid will be expanded for 100,000 people, the government will
cover premium costs for another 200,000 who buy private programs, while an
additional 200,000 will be required to buy insurance from low-cost policies
offered by private companies working in tandem with the government.
Romney signed the bill into law in April on the same Faneuil Hall stage where
Kerry planned his remarks.
Kerry
Proposes Universal Coverage by 2012, NYT, 31.7.2006,
http://www.nytimes.com/aponline/us/AP-Kerry-Health-Care.html
F.D.A. Plans to Consider Morning-After Pill
July 31, 2006
The New York Times
By JEREMY W. PETERS
The Food and Drug Administration said today it
is considering approval of the morning-after pill for sale without a
prescription, a surprise move on an issue that has ensnared the agency in debate
for years.
Discussions between the government and Barr Laboratories, which manufactures the
drug, known as Plan B, are set to begin immediately and could be completed “in a
matter of weeks,” the agency said in a statement.
The move could end a standoff between the Bush administration and Democrats on
Capitol Hill.
The decision to move forward with consideration of the pill, now available by
prescription, comes just as President Bush’s nominee to lead the F.D.A., Dr.
Andrew C. von Eschenbach, prepares to go before the Senate for his confirmation
hearings. Those hearings are to begin on Tuesday.
Approval of the nomination has been in doubt since Senators Hillary Rodham
Clinton of New York and Patty Murray of Washington, both Democrats who support
over-the-counter sales of Plan B, said they would block any vote on Dr. von
Eschenbach until the agency makes a decision.
Barr’s application for over-the-counter approval of Plan B has been pending
before the F.D.A. for three years and has sparked considerable discord within
the agency. It has also become a proxy fight in the debate between foes and
supporters of abortion rights.
In December 2003, an F.D.A. advisory committee voted 23 to 4 to approve Barr’s
application with no age restrictions. Six months later, however, a top agency
official rejected the application, citing concerns that the pill would be
available to young teenagers.
Barr resubmitted its application, this time seeking approval to sell the drug
only to those 16 and older.
Internal F.D.A. documents show that agency officials suggested to Barr that it
rewrite its application to allow over-the-counter sales to adult women while
still requiring younger teenagers to get a prescription. Barr did that, but in
January 2005, the statutory deadline for an F.D.A. decision passed without a
decision.
In a letter to Barr today, Dr. von Eschenbach indicated the F.D.A. would not
approve Plan B for over-the-counter sale for girls under 18. “We believe that
the appropriate age for OTC access is 18,” he wrote.
While the F.D.A. has insisted that its decisions to reject or delay the Plan B
application were the result of scientific or regulatory concerns, a
Congressional investigation found last year that top agency officials decided at
one point to reject the application before its staff’s scientific review was
even complete.
Dr. Susan Wood resigned in August as director of the F.D.A.’s office of women’s
health to protest what she said was political interference in the agency’s
scientific deliberations.
F.D.A. Plans to Consider Morning-After Pill, NYT, 31.7.2006,
http://www.nytimes.com/2006/07/31/giving/31cnd-pill.html?hp&ex=1154404800&en=3df0f0cc0e529b01&ei=5094&partner=homepage
The New Age
So Big and Healthy Nowadays That Grandpa
Wouldn’t Even Know You
July 30, 2006
The New York Times
By GINA KOLATA
Valentin Keller enlisted in an all-German unit
of the Union Army in Hamilton, Ohio, in 1862. He was 26, a small, slender man, 5
feet 4 inches tall, who had just become a naturalized citizen. He listed his
occupation as tailor.
A year later, Keller was honorably discharged, sick and broken. He had a lung
ailment and was so crippled from arthritis in his hips that he could barely
walk.
His pension record tells of his suffering. “His rheumatism is so that he is
unable to walk without the aid of crutches and then only with great pain,” it
says. His lungs and his joints never got better, and Keller never worked again.
He died at age 41 of “dropsy,” which probably meant that he had congestive heart
failure, a condition not associated with his time in the Army. His 39-year-old
wife, Otilia, died a month before him of what her death certificate said was
“exhaustion.”
People of Valentin Keller’s era, like those before and after them, expected to
develop chronic diseases by their 40’s or 50’s. Keller’s descendants had lung
problems, they had heart problems, they had liver problems. They died in their
50’s or 60’s.
Now, though, life has changed. The family’s baby boomers are reaching middle age
and beyond and are doing fine.
“I feel good,” says Keller’s great-great-great-grandson Craig Keller. At 45, Mr.
Keller says he has no health problems, nor does his 45-year-old wife, Sandy.
The Keller family illustrates what may prove to be one of the most striking
shifts in human existence — a change from small, relatively weak and sickly
people to humans who are so big and robust that their ancestors seem almost
unrecognizable.
New research from around the world has begun to reveal a picture of humans today
that is so different from what it was in the past that scientists say they are
startled. Over the past 100 years, says one researcher, Robert W. Fogel of the
University of Chicago, humans in the industrialized world have undergone “a form
of evolution that is unique not only to humankind, but unique among the 7,000 or
so generations of humans who have ever inhabited the earth.”
The difference does not involve changes in genes, as far as is known, but
changes in the human form. It shows up in several ways, from those that are well
known and almost taken for granted, like greater heights and longer lives, to
ones that are emerging only from comparisons of health records.
The biggest surprise emerging from the new studies is that many chronic ailments
like heart disease, lung disease and arthritis are occurring an average of 10 to
25 years later than they used to. There is also less disability among older
people today, according to a federal study that directly measures it. And that
is not just because medical treatments like cataract surgery keep people
functioning. Human bodies are simply not breaking down the way they did before.
Even the human mind seems improved. The average I.Q. has been increasing for
decades, and at least one study found that a person’s chances of having dementia
in old age appeared to have fallen in recent years.
The proposed reasons are as unexpected as the changes themselves. Improved
medical care is only part of the explanation; studies suggest that the effects
seem to have been set in motion by events early in life, even in the womb, that
show up in middle and old age.
“What happens before the age of 2 has a permanent, lasting effect on your
health, and that includes aging,” said Dr. David J. P. Barker, a professor of
medicine at Oregon Health and Science University in Portland and a professor of
epidemiology at the University of Southampton in England.
Each event can touch off others. Less cardiovascular disease, for example, can
mean less dementia in old age. The reason is that cardiovascular disease can
precipitate mini-strokes, which can cause dementia. Cardiovascular disease is
also a suspected risk factor for Alzheimer’s disease.
The effects are not just in the United States. Large and careful studies from
Finland, Britain, France, Sweden and the Netherlands all confirm that the same
things have happened there; they are also beginning to show up in the
underdeveloped world.
Of course, there were people in previous generations who lived long and healthy
lives, and there are people today whose lives are cut short by disease or who
suffer for years with chronic ailments. But on average, the changes, researchers
say, are huge.
Even more obvious differences surprise scientists by the extent of the change.
In 1900, 13 percent of people who were 65 could expect to see 85. Now, nearly
half of 65-year-olds can expect to live that long.
People even look different today. American
men, for example, are nearly 3 inches taller than they were 100 years ago and
about 50 pounds heavier.
“We’ve been transformed,” Dr. Fogel said.
What next? scientists ask. Today’s middle-aged people are the first generation
to grow up with childhood vaccines and with antibiotics. Early life for them was
much better than it was for their parents, whose early life, in turn, was much
better than it was for their parents.
And if good health and nutrition early in life are major factors in determining
health in middle and old age, that bodes well for middle-aged people today.
Investigators predict that they may live longer and with less pain and misery
than any previous generation.
“Will old age for today’s baby boomers be anything like the old age we think we
know?” Dr. Barker asked. “The answer is no.”
Trying to Change a Pattern
Craig Keller does not know what to expect of his old age. But he is optimistic
by nature, and he knows he has already lived past the life span of his
beleaguered ancestor Valentin. He is 5-foot-9, 200 pounds and exuberantly
healthy.
He grew up in Hamilton, the same town on the Kentucky border where Valentin
lived, worshiped and was buried. And he still lives there, working as a court
bailiff, married to Sandy, whom he met when they were in second grade. Now,
married 25 years, the Kellers have two grown daughters, a lively black dog and
no complaints.
Craig and Sandy Keller had all the advantages of middle-class Americans of their
age: childhood vaccines, plenty of food, antibiotics when they fell ill. Now,
wanting to stay healthy, they walk in the evenings, try to eat well and rely on
their strong faith, which, they say, makes a big difference to their health. And
they enjoy life.
Mr. Keller pulls his wife’s tan Chevy Malibu into the driveway of his small,
immaculate house on a sidewalk-lined street. It is the same house that he grew
up in; he and Mrs. Keller bought it from Mr. Keller’s parents 22 years ago.
While Mrs. Keller brings out a snack of a homemade cheese ball, crackers,
sandwiches, fruit salad and brownies, Mr. Keller settles in to marvel at the
contrast between his comfortable life and the lives of his ancestors.
For him, the idea of falling ill in his late 20’s and never working again is
unimaginable. He knows, though, that he is nearing the age when many of his
ancestors died. His father, Carl D. Keller, a lifelong smoker, developed
prostate cancer, then emphysema, and then lung cancer, which killed him at age
65. His father’s father, Carl W. Keller, also a smoker, died of cancer of the
esophagus just after he turned 69. His grandfather on his mother’s side died of
cirrhosis of the liver at 55; his grandmother died at 56 of breast cancer.
“They never got out of their 50’s and 60’s,” Mr. Keller said. “So that’s kind of
in the back of your mind.” He worries about his lungs, given his family history.
He had pneumonia once and has had bronchitis.
But, Mr. Keller reasons, he is so physically different from his ancestors — he
has never smoked and is so much healthier, so much better fed — that he really
thinks he will break the spell.
And if exercise is good for health, the Kellers certainly have exercised. Mr.
Keller displays a bookcase in their basement, crammed with athletic trophies.
Mrs. Keller’s are from baton twirling, Mr. Keller’s are from baseball,
basketball, softball and soccer. Their daughters, 19-year-old Rachel and
22-year-old Kristy, got theirs cheerleading.
Mrs. Keller said that when she was her daughters’ age, “I didn’t think about my
health very much.”
“But later in my 30’s and toward my 40’s,” she said, “I started to think about
it. You try to eat right, you try to exercise. And you do see your parents with
illnesses. And you wonder about yourself. My mom had a quadruple bypass when she
was 75, and she had to have a pacemaker after that. She’s now in her 80’s, but
you do wonder.”
Was it genetic destiny or health habits that caused her mother’s heart disease?
Mrs. Keller asks herself. Her mother smoked for more than a decade, finally
quitting with great difficulty before Mrs. Keller was born. “She said the Lord
helped her,” Mrs. Keller said.
Mrs. Keller has never smoked. Concerned about heart disease, she had her
cholesterol level tested a few years ago and now takes medication to lower it.
She walks at lunch with the women in her office and after dinner with her
husband.
Her daughter Rachel, petite and quiet with a quick smile, is already thinking
about her family’s medical history. She worries about heart disease, worries
about lung disease. She has already had her cholesterol level measured — it was
normal. And she is shocked when people her age start smoking.
“In high school, none of my friends smoked,” she said. “They came back from
their first year in college, and all of them did.”
“It’s hard to think about getting old when you’re young,” Rachel added. “But
when you see your family members — my grandpa died of lung cancer, my
grandparents on both sides had cancer. So it’s on my mind a lot of times.”
But still, the future is so distant it is almost unfathomable to her. “I wonder
what we’re going to be like when we’re old,” she mused.
Lives Plagued by Illness
Scientists used to say that the reason people are living so long these days is
that medicine is keeping them alive, though debilitated. But studies like one
Dr. Fogel directs, using records of of Union Army veterans, have led many to
rethink that notion.
The study involves a random sample of about 50,000 Union Army veterans. Dr.
Fogel compared those men, the first generation to reach age 65 in the 20th
century, with people born more recently.
The researchers focused on common diseases that are diagnosed in pretty much the
same way now as they were in the last century. So they looked at ailments like
arthritis, back pain and various kinds of heart disease that can be detected by
listening to the heart.
The first surprise was just how sick people were, and for how long.
Instead of inferring health from causes of death on death certificates, Dr.
Fogel and his colleagues looked at health throughout life. They used the daily
military history of each regiment in which each veteran served, which showed who
was sick and for how long; census manuscripts; public health records; pension
records; doctors’ certificates showing the results of periodic examinations of
the pensioners; and death certificates.
They discovered that almost everyone of the Civil War generation was plagued by
life-sapping illnesses, suffering for decades. And these were not some unusual
subset of American men — 65 percent of the male population ages 18 to 25 signed
up to serve in the Union Army. “They presumably thought they were fit enough to
serve,” Dr. Fogel said.
Even teenagers were ill. Eighty percent of the male population ages 16 to 19
tried to sign up for the Union Army in 1861, but one out of six was rejected
because he was deemed disabled.
And the Union Army was not very picky. “Incontinence of urine alone is not
grounds for dismissal,” said Dora Costa, an M.I.T. economist who works with Dr.
Fogel, quoting from the regulations. A man who was blind in his right eye was
disqualified from serving because that was his musket eye. But, Dr. Costa said,
“blindness in the left eye was O.K.”
After the war ended, as the veterans entered middle age, they were rarely spared
chronic ailments.
“In the pension records there were descriptions of hernias as big as
grapefruits,” Dr. Costa said. “They were held in by a truss. These guys were
continuing to work although they clearly were in a lot of pain. They just had to
cope.”
Eighty percent had heart disease by the time they were 60, compared with less
than 50 percent today. By ages 65 to 74, 55 percent of the Union Army veterans
had back problems. The comparable figure today is 35 percent.
The steadily improving health of recent generations shows up in population after
population and country after country. But these findings raise a fundamental
question, Dr. Costa said.
“The question is, O.K., there are these differences, and yes, they are big. But
why?” she said.
“That’s the million-dollar question,” said David M. Cutler, a health economist
at Harvard. “Maybe it’s the trillion-dollar question. And there is not a
received answer that everybody agrees with.”
Outgrowing the Past
Don Hotchkiss, a civil engineer in Las Vegas and a descendant of Civil War
veterans, is an avid Civil War re-enactor. Early on, he and his brother tried to
sleep in an exact replica of one of the old tents.
It was too small, Mr. Hotchkiss said. He is six feet tall and stocky. His
brother, a police officer in Phoenix, is thinner, but 6-foot-2. The tents were
made for men who were average size then. “In the past 145 years, we’ve ballooned
up,” Mr. Hotchkiss said.
At a recent meeting of a Las Vegas chapter of the Sons of Confederate Veterans,
eight burly men crowded into a library meeting room. All had experienced the
equivalent of the Civil War tent problem.
“At the re-enactments, all the directors, all the costume directors say the
re-enactors are just too darn big,” said George McClendon, a hefty 67-year-old
retired airline pilot.
Mr. McClendon is right. Men living in the Civil War era had an average height of
5-foot-7 and weighed an average of 147 pounds. That translates into a body mass
index of 23, well within the range deemed “normal.” Today, men average 5-foot-9½
and weigh an average of 191 pounds, giving them an average body mass index of
28.2, overweight and edging toward obesity.
Those changes, along with the great improvements in general health and life
expectancy in recent years, intrigued Dr. Costa. Common chronic diseases —
respiratory problems, valvular heart disease, arteriosclerosis, and joint and
back problems — have been declining by about 0.7 percent a year since the turn
of the 20th century. And when they do occur, they emerge at older ages and are
less severe.
The reasons, she and others are finding, seem to have a lot to do with
conditions early in life. Poor nutrition in early years is associated with short
stature and lifelong ill health, and until recently, food was expensive in the
United States and Europe.
Dr. Fogel and Dr. Costa looked at data on height and body mass index among Union
Army veterans who were 65 and older in 1910 and veterans of World War II who
were that age in the 1980’s. Their data relating size to health led them to a
prediction: the World War II veterans should have had 35 percent less chronic
disease than the Union Army veterans. That, they said, is exactly what happened.
They also found that diseases early in life left people predisposed to chronic
illnesses when they grew older.
“Suppose you were a survivor of typhoid or tuberculosis,” Dr. Fogel said. “What
would that do to aging?” It turned out, he said, that the number of chronic
illnesses at age 50 was much higher in that group. “Something is being
undermined,” he said. “Even the cancer rates were higher. Ye gods. We never
would have suspected that.”
Men who had respiratory infections or measles tended to develop chronic lung
disease decades later. Malaria often led to arthritis. Men who survived
rheumatic fever later developed diseased heart valves.
And stressful occupations added to the burden on the body.
People would work until they died or were so disabled that they could not
continue, Dr. Fogel said. “In 1890, nearly everyone died on the job, and if they
lived long enough not to die on the job, the average age of retirement was 85,”
he said. Now the average age is 62.
A century ago, most people were farmers, laborers or artisans who were exposed
constantly to dust and fumes, Dr. Costa said. “I think there is just this
long-term scarring.”
Searching for Answers
Dr. Barker of Oregon Health and Science University is intrigued by the puzzle of
who gets what illness, and when.
“Why do some people get heart disease and strokes and others don’t?” he said.
“It’s very clear that current ideas about adult lifestyles go only a small way
toward explaining this. You can say that it’s genes if you want to cease
thinking about it. Or you can say, When do people become vulnerable during
development? Once you have that thought, it opens up a whole new world.”
It is a world that obsesses Dr. Barker. Animal studies and data that he and
others have been gathering have convinced him that health in middle age can be
determined in fetal life and in the first two years after birth.
His work has been controversial. Some say that other factors, like poverty, may
really be responsible. But Dr. Barker has also won over many scientists.
In one study, he examined health records of 8,760 people born in Helsinki from
1933 to 1944. Those whose birth weight was below about six and a half pounds and
who were thin for the first two years of life, with a body mass index of 17 or
less, had more heart disease as adults.
Another study, of 15,000 Swedish men and women born from 1915 to 1929, found the
same thing. So did a study of babies born to women who were pregnant during the
Dutch famine, known as the Hunger Winter, in World War II.
That famine lasted from November 1944 until May 1945. Women were eating as
little as 400 to 800 calories a day, and a sixth of their babies died before
birth or shortly afterward. But those who survived seemed fine, says Tessa J.
Roseboom, an epidemiologist at the University of Amsterdam, who studied 2,254
people born at one Dutch hospital before, during and after the famine. Even
their birth weights were normal.
But now those babies are reaching late middle age, and they are starting to get
chronic diseases at a much higher rate than normal, Dr. Roseboom is finding.
Their heart disease rate is almost triple that of people born before or after
the famine. They have more diabetes. They have more kidney disease.
That is no surprise, Dr. Barker says. Much of the body is complete before birth,
he explains, so a baby born to a pregnant woman who is starved or ill may start
life with a predisposition to diseases that do not emerge until middle age.
The middle-aged people born during the famine also say they just do not feel
well. Twice as many rated their health as poor, 10 percent compared with 5
percent of those born before or after the famine.
“We asked them whether they felt healthy,” Dr. Roseboom said. “The answer to
that tends to be highly predictive of future mortality.”
But not everyone was convinced by what has come to be known as the Barker
hypothesis, the idea that events very early in life affect health and well-being
in middle and old age. One who looked askance was Douglas V. Almond, an
economist at Columbia University.
Dr. Almond had a problem with the studies. They were not of randomly selected
populations, he said, making it hard to know if other factors had contributed to
the health effects. He wanted to see a rigorous test — a sickness or a
deprivation that affected everyone, rich and poor, educated and not, and then
went away. Then he realized there had been such an event: the 1918 flu.
The flu pandemic arrived in the United States in October 1918 and was gone by
January 1919, afflicting a third of the pregnant women in the United States.
What happened to their children? Dr. Almond asked.
He compared two populations: those whose mothers were pregnant during the flu
epidemic and those whose mothers were pregnant shortly before or shortly after
the epidemic.
To his astonishment, Dr. Almond found that the children of women who were
pregnant during the influenza epidemic had more illness, especially diabetes,
for which the incidence was 20 percent higher by age 61. They also got less
education — they were 15 percent less likely to graduate from high school. The
men’s incomes were 5 percent to 7 percent lower, and the families were more
likely to receive public assistance.
The effects, Dr. Almond said, occurred in whites and nonwhites, in rich and
poor, in men and women. He convinced himself, he said, that there was something
to the Barker hypothesis.
Craig Keller hopes it is true. He looks back at the hard life of his ancestors,
even those of his great-grandfather and his grandfather, working as painters,
exposed to fumes. And, of course, there was poor Valentin Keller, his Civil War
ancestor, his health ruined by the time he was 30.
Today, Mr. Keller says, he is big and healthy, almost despite himself. He would
like to think it is because he tries to live well, but he is not so sure,
especially when he hears about what Dr. Barker and Dr. Fogel and the others have
found. Maybe it was his good fortune to have been born to a healthy mother and
to be well fed and vaccinated.
“I don’t know if we have as much control as we think we do,” he said.
So
Big and Healthy Nowadays That Grandpa Wouldn’t Even Know You, NYT, 30.7.2006,
http://www.nytimes.com/2006/07/30/health/30age.html?hp&ex=1154232000&en=a8f44bc2e9318699&ei=5094&partner=homepage
Living Large and Healthy, but How Long Can
It Go On?
July 30, 2006
The New York Times
By GINA KOLATA
Longer life. Less disease. Less disability.
The trends have continued for more than a century as humans have become bigger,
stronger and healthier. But can they — will they — keep going? Or is there some
countertrend, obesity or an overuse of medications, perhaps, that will turn the
statistics around?
The questions are serious, but, researchers say, for now there are no easy
answers, only lessons in humility as, over and over again in recent years,
scientists have seen their best predictions overthrown.
Life expectancy, for example, has been a real surprise, says Eileen M. Crimmins,
a professor of gerontology and demographic research at the University of
Southern California. “When I came of age as a professional, 25 years ago,
basically the idea was three score years and 10 is what you get,” Dr. Crimmins
said. Life span was “this rock, and you can’t touch it.”
“But,” she added, “then we started noticing that in fact mortality is
plummeting.”
Will it continue much longer?
“It is an extremely controversial area, and the answer is, We don’t know,” said
Dr. Richard J. Hodes, director of the National Institute on Aging.
Some worry, for example, that today’s fat children will grow up to be tomorrow’s
heart disease and diabetes patients, destroying the nation’s gains in health and
well-being.
“It is very legitimate to be concerned about levels of overweight and obesity in
kids,” said David Williamson, a senior biomedical research scientist at the
Centers for Disease Control and Prevention. “But at the same time, those levels
of obesity are overlaid on improvements in health in children, which also affect
long-term health and longevity.”
An Uncertain Future
The mixed picture has led to disparate views about what is likely to occur.
S. Jay Olshansky, a professor of epidemiology and biostatistics at the
University of Illinois at Chicago, predicted in The New England Journal of
Medicine that obesity would lead to so much diabetes and heart disease that life
expectancy would “level off or even decline within the first half of this
century.”
Dr. Olshansky was countered by Samuel H. Preston, a professor of demography at
the University of Pennsylvania. Dr. Preston cited the population’s overall
better health, from childhood on, and said that obesity had already been
factored into national projections of life spans and that the projections were
that life spans would continue to increase.
Dana Goldman, director and corporate chairman of health economics at the RAND
Corporation, looked at the obesity question from another perspective:
disability. In a recent paper in Health Affairs, Dr. Goldman and his colleagues
reported that disability rates among young people had begun to increase,
although they continued to decline for the elderly. He suspects it is because of
obesity and says it does not auger well.
He said in a telephone interview that the increased number of disabled involved
less than 1 percent of young people. That means it is possible that he is seeing
a spurious trend resulting from minor changes in reporting practices.
“I think of this as the ‘storm clouds on the horizon’ phenomenon,” Dr. Goldman
said.
Others remain circumspect. Perhaps obesity will lead to increased disability,
some say. While disability is declining over all, said Dr. Richard M. Suzman,
director of the office of behavioral and social research programs at the
National Institute on Aging, “if you hadn’t had the increase in obesity, would
disability have gone down much faster?”
The problem for now, Dr. Williamson says, is that there is so much concern over
obesity that other factors may be ignored.
He tells of a recent episode that illustrates his point, when he went with some
Italian colleagues to see a photography exhibit.
“We were looking at pictures of Pennsylvania coal miners in the late 1800’s and
early 1900’s,” Dr. Williamson said. “A lot of these people were kids.”
“The Italians said to me, ‘Oh, look. These kids were so thin.’ ”
“I said, ‘Well, hell yes they were thin. But were they healthy?’ ” It is likely
that they were poor, malnourished and sick from the coal dust, he added. No
wonder they were thin.
“It really got me thinking about, gosh, have we gotten so out of touch?” Dr.
Williamson said. Obesity, he said, is a very legitimate concern, but it is not
the only health risk. And being thin does not necessarily equate with being
healthy.
Living Large and Healthy, but How Long Can It Go On?, NYT, 30.7.2006,
http://www.nytimes.com/2006/07/30/health/30ageside.html
Senate Removes Abortion Option for Young
Girls
July 26, 2006
The New York Times
By CARL HULSE
WASHINGTON, July 25 — The Senate passed
legislation Tuesday that would make it a federal crime to help an under-age girl
escape parental notification laws by crossing state lines to obtain an abortion.
The bill was approved on a 65-to-34 vote, with 14 Democrats joining 51
Republicans in favor.
A similar measure passed the House last year, and President Bush said he would
sign the legislation if the two chambers could work out their differences and
send a final bill to him.
In a statement, Mr. Bush said that “transporting minors across state lines to
bypass parental consent laws regarding abortion undermines state law and
jeopardizes the lives of young women.”
Critics questioned the necessity of the measure, saying it would apply to only a
small number of cases and could result in criminal charges against close
relatives or clergy members who interceded to help in a time of personal crisis.
Proponents of the bill, acknowledging that it was unknown how often such
incidents occurred, said abortion clinics in states without such parental
involvement laws had advertised that no consent was needed in an effort to
appeal to those interested in avoiding such requirements.
“If they are advertising, then it obviously at least happens,” said Senator John
Ensign, the Nevada Republican who wrote the measure. “If it is happening 20
times a year, it is still worth doing to protect those parental rights and to
protect those children from being in these kinds of situations.”
The legislation is the latest in a push by anti-abortion forces to seek
incremental changes in federal laws rather than press for a broad rollback of
abortion rights.
The measure also provided Republicans another opportunity to reassure their
social conservative base that its concerns were being addressed in an election
year. And it gave them a chance to force Democrats to take a position on an
issue some would prefer to avoid out of concern over alienating abortion-rights
advocates on one hand or Democratic centrists on the other.
Twenty-nine Democrats, four Republicans and one independent voted against the
bill. Polls have shown consistently that notification requirements are popular
with parents. Advocates of the bill said most Americans shared the view that
parents should be consulted when it comes to such a consequential matter in the
life of a teenager.
“What opponents of this bill forget is that no parent wants anyone to take their
children across state lines — or even across the street — without their
permission,” said Senator Mitch McConnell of Kentucky, the No. 2 Republican in
the Senate.
Opponents said cases would inevitably arise in which a girl had been victimized
by a relative, or in which parents were not available or did not have the girl’s
best interest in mind. In those cases, they said, the legislation will pose a
hardship or worse.
“Life is not always the way we wish it to be,” said Senator Hillary Rodham
Clinton, Democrat of New York, who opposed the bill. “Sometimes tragedies
happen, and sometimes families are not just negligent but abusive, and sometimes
young girls are taken advantage of by members of their family, people in whom
they should be able to trust.”
Others were pushing the measure to provide an opportunity for some lawmakers who
are against abortion to make political amends after voting last week to support
expanding federal research using embryonic stem cells. They said the measure
could penalize close relatives trying to come to the aid of a child in trouble,
who was the victim of incest or feared a physically violent response to the
revelation of a pregnancy.
“I don’t think the American people support throwing Grandma in jail because she
embraced her granddaughter and said, ‘Oh my God, I’m worried that your dad may
hurt you if you tell the truth,’ ” said Senator Barbara Boxer, Democrat of
California.
Under the legislation, known officially as the Child Custody Protection Act,
those found guilty of violating it would be subject to a fine and up to a year
in jail. Douglas Johnson, the legislative director of the National Right to Life
Committee, said the provisions would apply to 26 states that have enforceable
laws requiring minor girls to notify or receive the consent of their parents or
seek approval from a judge before seeking an abortion.
Mr. Johnson said there “is evidence of widespread circumvention of these state
notification laws,” though the frequency varies around the nation depending on
the proximity of states without such restrictions. He said anecdotal accounts
suggested that many cases involved under-age girls and older men.
Those challenging the measure said they believed that the number of those who
went out of state specifically to avoid parental notification laws was low. They
said Congress should instead focus on sex education and counseling. A proposal
to create new pregnancy prevention grants was defeated on a 51-to-48 vote.
“The American public wants teen pregnancy prevented, not punished,” said Nancy
Keenan, president of Naral Pro-Choice America. “This bill does nothing to
protect young people or promote communication between teens and their parents.”
To stem criticism that the measure protected fathers guilty of incest,
Republicans joined Democrats in approving an amendment that says a parent who
has committed incest and transports a minor out of state for an abortion will
also face a fine and jail time.
The chief difference between the House and Senate bills is that the House
measure requires an out-of-state doctor to provide 24 hours’ notice to a girl’s
parents or face criminal penalties. Parents can also sue the person performing
the abortion.
Despite the strong vote for the measure, the Democratic leadership objected
Tuesday night to a Republican call to appoint negotiators to begin reconciling
the House and Senate bills, showing that Democrats were not going to make it
easy to reach a final deal.
Senate Removes Abortion Option for Young Girls, NYT, 26.7.2006,
http://www.nytimes.com/2006/07/26/washington/26abort.html?hp&ex=1153972800&en=8f98475eee481bc4&ei=5094&partner=homepage
Scientists Say They’ve Found a Code Beyond
Genetics in DNA
July 25, 2006
The New York Times
By NICHOLAS WADE
Researchers believe they have found a second
code in DNA in addition to the genetic code.
The genetic code specifies all the proteins that a cell makes. The second code,
superimposed on the first, sets the placement of the nucleosomes, miniature
protein spools around which the DNA is looped. The spools both protect and
control access to the DNA itself.
The discovery, if confirmed, could open new insights into the higher order
control of the genes, like the critical but still mysterious process by which
each type of human cell is allowed to activate the genes it needs but cannot
access the genes used by other types of cell.
The new code is described in the current issue of Nature by Eran Segal of the
Weizmann Institute in Israel and Jonathan Widom of Northwestern University in
Illinois and their colleagues.
There are about 30 million nucleosomes in each human cell. So many are needed
because the DNA strand wraps around each one only 1.65 times, in a twist
containing 147 of its units, and the DNA molecule in a single chromosome can be
up to 225 million units in length.
Biologists have suspected for years that some positions on the DNA, notably
those where it bends most easily, might be more favorable for nucleosomes than
others, but no overall pattern was apparent. Drs. Segal and Widom analyzed the
sequence at some 200 sites in the yeast genome where nucleosomes are known to
bind, and discovered that there is indeed a hidden pattern.
Knowing the pattern, they were able to predict the placement of about 50 percent
of the nucleosomes in other organisms.
The pattern is a combination of sequences that makes it easier for the DNA to
bend itself and wrap tightly around a nucleosome. But the pattern requires only
some of the sequences to be present in each nucleosome binding site, so it is
not obvious. The looseness of its requirements is presumably the reason it does
not conflict with the genetic code, which also has a little bit of redundancy or
wiggle room built into it.
Having the sequence of units in DNA determine the placement of nucleosomes would
explain a puzzling feature of transcription factors, the proteins that activate
genes. The transcription factors recognize short sequences of DNA, about six to
eight units in length, which lie just in front of the gene to be transcribed.
But these short sequences occur so often in the DNA that the transcription
factors, it seemed, must often bind to the wrong ones. Dr. Segal, a
computational biologist, believes that the wrong sites are in fact inaccessible
because they lie in the part of the DNA wrapped around a nucleosome. The
transcription factors can only see sites in the naked DNA that lies between two
nucleosomes.
The nucleosomes frequently move around, letting the DNA float free when a gene
has to be transcribed. Given this constant flux, Dr. Segal said he was surprised
they could predict as many as half of the preferred nucleosome positions. But
having broken the code, “We think that for the first time we have a real
quantitative handle” on exploring how the nucleosomes and other proteins
interact to control the DNA, he said.
The other 50 percent of the positions may be determined by competition between
the nucleosomes and other proteins, Dr. Segal suggested.
Several experts said the new result was plausible because it generalized the
longstanding idea that DNA is more bendable at certain sequences, which should
therefore favor nucleosome positioning.
“I think it’s really interesting,” said Bradley Bernstein, a biologist at
Massachusetts General Hospital.
Jerry Workman of the Stowers Institute in Kansas City said the detection of the
nucleosome code was “a profound insight if true,” because it would explain many
aspects of how the DNA is controlled.
The nucleosome is made up of proteins known as histones, which are among the
most highly conserved in evolution, meaning that they change very little from
one species to another. A histone of peas and cows differs in just 2 of its 102
amino acid units. The conservation is usually attributed to the precise fit
required between the histones and the DNA wound around them. But another reason,
Dr. Segal suggested, could be that any change would interfere with the
nucleosomes’ ability to find their assigned positions on the DNA.
In the genetic code, sets of three DNA units specify various kinds of amino
acid, the units of proteins. A curious feature of the code is that it is
redundant, meaning that a given amino acid can be defined by any of several
different triplets. Biologists have long speculated that the redundancy may have
been designed so as to coexist with some other kind of code, and this, Dr. Segal
said, could be the nucleosome code.
Scientists Say They’ve Found a Code Beyond Genetics in DNA, NYT, 25.7.2006,
http://www.nytimes.com/2006/07/25/science/25dna.html
Stem Cell Work Gets States’ Aid After Bush
Veto
July 25, 2006
The New York Times
By JODI RUDOREN
CHICAGO, July 24 — President Bush’s veto of
legislation to expand federally financed embryonic stem cell research has had
the unintended consequence of drawing state money into the contentious field and
has highlighted the issue in election campaigns across the country.
Two governors seized the political moment Thursday, the day after the veto, to
raise their ante for stem cell research.
Gov. Arnold Schwarzenegger of California, a Republican who helped Mr. Bush win a
second term but has long disagreed with him on this research, cited the veto as
he lent $150 million from the state’s general fund to pay for grants to stem
cell scientists. In Illinois, Gov. Rod R. Blagojevich, a Democrat opposed to
most every White House initiative, offered $5 million for similar grants in his
state.
Before the announcements, the only money available was $72 million that five
states had allocated for the research and $90 million that the National
Institutes of Health had provided since 2001 for work on a restricted number of
stem cell lines.
Several other governors, including one Republican, M. Jodi Rell of Connecticut,
denounced the president’s veto, his first, in a sign of the political potency of
the stem cell debate.
Within hours, too, the issue sprang to the forefront of some crucial campaigns,
including ones for governor, senator and representative in Colorado, Florida,
Maryland, Missouri and Tennessee.
In many cases, Republican moderates, mindful of consistent polls showing public
support for expanded stem cell research and expecting the promised attacks from
Democrats, sought to distinguish their positions from their president’s.
For Mr. Schwarzenegger, who is running for re-election in a state dominated by
Democrats, support for stem cell research has helped position him as a centrist,
but his Democratic opponent, Phil Angelides, the state treasurer, tried to
one-up him by taking credit for the loan.
Sean Tipton, president of the Coalition for the Advancement of Medical Research,
the lead lobbyist for the bill Mr. Bush vetoed, said, “In terms of actually
getting some resources to the scientists, it turns out like it may be a good
week.”
“I also think there’s symbolic significance,” Mr. Tipton said. “It sends a
strong signal to patients that there are some politicians that care about them
and want to see them taken care of.”
Tony Snow, the White House press secretary, said of the president, “While he
recognizes that states have the legal power to use their own funds for embryonic
stem cell research, he hopes researchers and entrepreneurs will focus on
developing effective cures,” including those “that don’t involve controversial
practices.”
Douglas Johnson of the National Right to Life Committee dismissed the
initiatives in Illinois and California as a “public relations gimmick” to divert
attention from a debate over whether scientists should be allowed to create
embryos through cloning.
“It’s regrettable,” Mr. Johnson said, “but it’s really a matter of their trying
to focus public attention on an issue that is significant but is not really the
front line of this battle.”
In Florida, stem cell research is a rare point of contention between two
Republicans vying to succeed the president’s brother Jeb as governor. But when
one of them, Attorney General Charlie Crist, announced that he “respectfully”
disagreed with the veto, his rival Tom Gallagher, the chief financial officer,
accused Mr. Crist of taking “every opportunity to disagree with the governor and
the mainstream of the party.”
Meanwhile, Rod Smith, the Florida state senator who is the Democratic candidate
for governor, promised, “When I become governor, we are absolutely going to do
stem cell research and we are going to fund it in this state.”
In Maryland, Democratic hopefuls in the governor’s race responded to the veto
with visits to the homes of quadriplegics and patients with Parkinson’s disease
who could benefit from stem cell research, while the Republican incumbent, Gov.
Robert L. Ehrlich Jr., pointed to his support of the research as evidence that
he did not “govern from the right or the left but the center, where most of us
are.”
In Colorado, Representative Diana DeGette, a Democrat and a sponsor of the
vetoed legislation, staged a protest rally on Friday when the president visited
her district for a $1,000-a-plate luncheon on behalf of Rick O’Donnell, a
Republican who supports his position.
Nowhere is the issue hotter than in Missouri, where voters in November are
likely to face a ballot initiative supporting stem cell research, and where
Senator Jim Talent, a Republican who is seeking re-election, opposes it. Mr.
Talent’s Democratic challenger, Claire McCaskill, the state auditor, highlighted
the issue last week when she delivered the Democrats’ radio address and then
initiated a conference call with national reporters to spotlight her support.
The moves in California and Illinois continue the patchwork pattern of public
financing for stem cell research since 2001, when Mr. Bush announced his policy
restricting how federal money could be used in the arena.
More than 100 bills have been considered over the past two years by dozens of
state legislatures, with one, South Dakota’s, banning such research altogether
and five — in California, Connecticut, Illinois, Maryland and New Jersey —
allocating state resources to the effort. Other states, including Indiana,
Massachusetts, Virginia and Wisconsin, have taken steps to support stem cell
science without directly paying for research, while Arizona, North Carolina and
Virginia have formed groups to study their state’s role in the emerging field.
Mr. Schwarzenegger’s announcement on Thursday of the $150 million loan will
provide the single largest public pot yet available.
“I think with one stroke, the president energized” the program, said Zach W.
Hall, the president of the California Institute for Regenerative Medicine, which
had an anemic $14 million to spread among 16 training grants before the veto,
and which will soon be flush. “It’s not what we would have wanted, but it did
have that beneficent side effect.”
For California, the $150 million is half the $300 million per year that would be
provided under a decade-long, $3 billion bond issue that 59 percent of voters
approved in 2004. Taxpayer groups sued to block the bonds and appealed a verdict
in May that favored the state. At the same time, “bond anticipation notes”
floated in the interim found little favor in the market. The $150 million loan
is intended to fill that shortfall and would be repaid by bond proceeds,
presuming the state prevails in court.
“Arnold is supposed to be a Republican, so I don’t understand his thinking here
with President Bush. It seems like he’s going against the party line,” said Dana
Cody, executive director of the Life Legal Defense Foundation, one of the groups
suing the state. “It’s very inconsistent with the governor’s platform, if you
will, of ‘we’re tired of being taxed.’ That’s $150 million coming out of the
taxpayers’ pocket for something that is questionable at best because of the
litigation.”
Asked at a news conference in Sacramento on Friday about the political
implications of making such a forceful public move to oppose the president he
has previously supported, Mr. Schwarzenegger said, “You don’t have to agree with
someone on every issue.”
“It doesn’t matter to me what the president thinks about it, or what any party
thinks about it,” the governor added. “I always try to do what’s best for the
people of California.”
In Illinois, the $5 million would come out of the administrative budget in the
Department of Healthcare and Family Services, and would be added to $10 million
in grants awarded in April to hospitals and universities. A five-year, $100
million investment that Mr. Blagojevich pushed has been stalled in the
Legislature.
Mr. Blagojevich, who was vacationing in Michigan when the new money was
announced via a news release, declined an interview request, through a
spokeswoman, Abby Ottenhoff.
“It was after the veto that the governor determined there were no more options,”
Ms. Ottenhoff said. “This research is too important to put on hold until there
is a new leader in the White House.”
Even with the limitations on federal financing, the overall financing available
for stem cell research could be described as fairly robust, given that the
research is still at a basic stage and that in addition to state money,
philanthropies like the Howard Hughes Medical Institute have made contributions.
Moreover, in the private sector, biotech companies like Geron, Advanced Cell
Technology and Athersys conduct research on embryonic or adult stem cells.
While stem cell scientists applauded the states’ efforts, they cautioned that
such an approach was not ideal.
“In the long term, I don’t think it’s a good idea to have individual states
trying to mount efforts which are going to be more piecemeal, less effective and
take more time than a federal effort,” said Douglas A. Melton, co-director of
the Stem Cell Institute at Harvard University. “I don’t think states should
mount their own militias either.”
Dr. Arnold Kriegstein, director of the Institute for Regeneration Medicine at
the University of California, San Francisco, said that the $150 million was
“absolutely a boon,” but that “if you’re an investigator in another state,
besides Illinois or California, I think you’d be very frustrated right now.”
Candace Coffee, a Los Angeles resident who has suffered partial blindness,
paralysis and constant headaches from Devic’s disease, appeared with Governor
Schwarzenegger on Friday at his news conference.
“President Bush’s veto stole my hope,” Ms. Coffee said. “But just as quickly as
our hope was stolen, it was renewed.”
Stem
Cell Work Gets States’ Aid After Bush Veto, NYT, 25.7.2006,
http://www.nytimes.com/2006/07/25/us/25stem.html?hp&ex=1153886400&en=0a4ddc283632d4a8&ei=5094&partner=homepage
Catholic Group Urges Candidates to Return
Cash
July 25, 2006
The New York Times
By STEPHANIE STROM
The Missouri Catholic Conference is urging
candidates for state offices to return contributions from a nonprofit
organization that advocates for stem cell research and other medical analysis
and testing.
The request has inspired a complaint to the Internal Revenue Service, arguing
that it violates prohibitions on political activity by nonprofit organizations.
“It constitutes illegal political interference,” said Marcus S. Owens, a tax
lawyer, who filed the complaint on behalf of a client he declined to identify.
The Missouri conference sent the request to more than 50 candidates for state
offices who received donations from the organization, Supporters of Health
Research and Treatments.
Lawrence A. Weber, executive director and general counsel of the Missouri
conference, said he heard about the complaint over the weekend but did not see
Mr. Owens’s letter until a reporter faxed it to him on Monday.
“Obviously, it’s something we take seriously and are in the process of looking
into,” Mr. Weber said.
Representatives for Supporters of Health Research could not be reached.
Missouri legislators are considering an amendment to the State Constitution that
would ban human cloning but would prohibit the state and local governments from
discouraging stem cell research, which is allowed under federal law.
The Missouri conference opposes that amendment. In April, Mr. Weber sent a
letter to several dozen state legislators who were reported to have received
campaign contributions from Supporters of Health Research.
“The Missouri Catholic Conference is committed to informing Missouri voters
about campaign contributions promoting human cloning and embryonic stem cell
research,” Mr. Weber wrote, “and will report to Missouri voters regarding
candidates who choose to associate themselves with this and similar
organizations that promote such unethical practices.”
He added that if candidates returned contributions from Supporters of Health
Research, the conference would report that to diocesan newspapers so long as
documentation was provided.
This month, the St. Louis Review Online, a diocesan Web site, reported that
eight candidates had returned money to organizations that support stem cell
research. On Monday, Mr. Weber said that “quite a few” candidates had returned
such contributions.
State Representative Jim Guest, a Republican from northwest Missouri, said he
was stunned by the letter’s tone. “I’m not sure if extortion is the right word,”
Mr. Guest said, “but they basically threatened me if I didn’t return the money,
and that’s certainly stepping across the line.”
Mr. Guest has not returned the money. “I was going to work for the issue anyway,
but it almost made me feel like working harder,” he said.
Catholic Group Urges Candidates to Return Cash, NYT, 25.7.2006,
http://www.nytimes.com/2006/07/25/washington/25threat.html?_r=1&oref=slogin
Senate to Pass Parental Notification Law
July 25, 2006
By THE ASSOCIATED PRESS
Filed at 3:44 a.m. ET
The New York Times
WASHINGTON (AP) -- A pregnant 14-year-old from
Lancaster, Pa., decides to keep and raise her baby. Her boyfriend's parents
drive her to a New Jersey abortion clinic to get around her home state's
parental notification law. They then refuse to take her home until she ends her
pregnancy.
It happened -- and a national parental notification law could have stopped it,
the girl's mother, Marcia Carroll, told a House panel last year.
A year after the House passed the measure, a similar version is heading toward
Senate approval Tuesday with widespread public support.
Opponents, however, say the legislation would cut off an escape route for
pregnant teens with abusive parents and punish confidants who might try to help
them.
''We should not criminalize the grandparents or clergy members to whom a teen in
trouble might turn for help,'' said Sen. Dianne Feinstein, D-Calif., who will
introduce an amendment to protect such confidants from prosecution.
No one knows exactly how many girls try to cross state lines to end pregnancies
to circumvent parental notification and consent laws back home.
Polls suggest there is widespread public backing for the bill, with almost
three-quarters of respondents saying a parent has the right to give consent
before a child under 18 has an abortion.
''This is clearly not an issue divided on pro-life or pro-choice lines,'' said
Sen. John Ensign, R-Nev., the bill's original sponsor. ''There is broad and
consistent support to preserve the rights of parents.''
Under the bill, anyone who helps a pregnant minor cross state lines to obtain an
abortion without the knowledge of her parents could be punished by unspecified
fines and up to a year in prison. The girl and her parents would not be
vulnerable to criminal penalties. The measure contains an exception for those
who help underage girls get such abortions to avoid life-threatening conditions.
Democrats will present several other amendments, including one that would add
exceptions for anyone helping girls to end pregnancies resulting from rape or
incest.
The states without parental notification or consent laws are: Washington,
Oregon, New York, Vermont, Rhode Island, and Connecticut, plus the District of
Columbia.
The bill passed the House 270-157 in April 2005 after lawmakers rejected an
amendment similar to Feinstein's.
The bills are S. 403 and H.R. 748.
------
On the Net:
Congress: http://thomas.loc.gov
Senate to Pass Parental Notification Law, NYT, 25.7.2006,
http://www.nytimes.com/aponline/us/AP-Interstate-Abortion.html
HCA Buyout Highlights Era of Going Private
July 25, 2006
The New York Times
By ANDREW ROSS SORKIN
In April, investment bankers from Merrill
Lynch paid one of their regular visits to HCA, the hospital company. Instead of
the usual pitch to sell HCA some more hospitals, the bankers had a more
audacious proposal: Assemble a group of private investors to acquire the company
for more than $30 billion.
Yesterday, HCA agreed to do just that, to sell itself to three private-equity
firms and the family of Senator Bill Frist, the Senate majority leader, whose
father, the late Dr. Thomas Frist Sr., and his brother, Dr. Thomas F. Frist Jr.,
founded HCA.
The deal, including debt, is the largest leveraged buyout, eclipsing the $30.6
billion takeover of RJR Nabisco in 1989.
If that 1980’s deal came to define an era — as depicted in the book “Barbarians
at the Gate’’ — and helped usher in the modern private-equity industry, the deal
yesterday crowns private equity’s ascension to the top of finance: the
“barbarians’’ now rule the deal world.
Private-equity firms like Kohlberg Kravis Roberts, which came to fame in the RJR
buyout, and others largely unknown outside Wall Street now possess more than $2
trillion in buying power. In addition to Kohlberg Kravis, the new brand names of
finance are Bain Capital, Blackstone Group, Carlyle Group and Texas Pacific
Group. The companies they own include Toys “R’’ Us and Hertz.
The deal-making prowess of the big private-equity firms means that they have
become Wall Street’s most important clients. Beyond Wall Street, the role of
private equity as an investor has reshaped industries from energy to retailing
to Hollywood.
The buyout spree is expected to run on. Some big public companies, fed up with
scrutiny from investors and regulators, are now selling themselves to
private-equity firms. And private equity is increasingly able to take on bigger
deals. Firms raised more than $260 billion worldwide just this year from big
money managers like pension funds and university endowments. This month,
Blackstone Group raised $15.6 billion, creating the world’s largest
private-equity fund.
“I get calls all the time from C.E.O.’s,’’ said Cristóbal I. Conde, chief
executive of SunGard Data Systems, which was acquired by a group of
private-equity firms last year for $11.3 billion. “They think they need to
consider going private. They can’t ignore the possibility anymore.”
Private-equity firms use the money they have raised and borrow more to buy
businesses. The firms borrow against the value of the asset and the cash flow of
the company they are acquiring, often allowing the firms to invest only a small
sum of equity in a large transaction.
In the HCA deal, the three private-equity firms — Bain, Kohlberg Kravis and
Merrill Lynch’s buyout unit — and the Frist family are investing only $5.5
billion in cash. The rest of the $31.6 billion price tag is being financed by
debt, which the firms will hope to pay down, like a mortgage payment, using
HCA’s income.
Aided by relatively cheap borrowing costs, private-equity firms have gone on a
shopping spree. This year they have bought some of the world’s best-known
brands, worth more than $347 billion, twice last year’s pace and roughly equal
to the gross domestic product of Belgium. Private-equity firms spent $12.3
billion for Univision last month; $22 billion for Kinder Morgan in May; as much
as $14 billion for General Motors’ finance unit, G.M.A.C., in April; and $17.4
billion for Albertsons, the grocery chain, in January.
Not only has the size and breadth of private equity deals mushroomed, but the
tactics of the firms when they win control of companies have changed
substantially. For years, private-equity firms had reputations as corporate
raiders that would come into companies and slash and burn jobs to reduce costs.
Today, cutting costs is not private equity’s only approach. Indeed, since
SunGard agreed to be acquired, it has added 3,000 jobs.
Many of the recent successes of private-equity firms have been tied to their
abilities to pile more debt on the businesses than many public investors feel
comfortable with.
“The rise of private equity has been a function of the confidence that the
equity markets and debt markets have in the management of these firms,” said
David M. Rubenstein, the co-founder of Carlyle Group, who is currently working
on a book tentatively titled “Beyond Wall Street.”
Mr. Conde of SunGard said: “When you’re running a public company so much of your
credibility is linked to the volatility of your earnings. Whether you’re up by a
penny or you’re down by a penny is a big deal. As a private company, we can
tolerate more volatility.”
The rise of private equity, however, raises questions for public investors, who
have often sold businesses only to see them resold, at enormous profits, just
years later by the private firms. Hertz, for example, which was acquired late
last year from Ford by a group of private-equity firms, is now seeking a public
listing less than eight months after the original deal was reached. The equity
firms increased Hertz’s debt, paid themselves a $1 billion special dividend, and
made some performance improvements.
H. J. Heinz is under attack by some shareholders for selling Weight Watchers in
1999 for $735 million. The firms that bought Weight Watchers retooled the
business; after becoming a private company and being taken public, it is worth
$4.2 billion.
At a meeting at the World Economic Forum in Davos, Switzerland, this year,
Daniel Loeb, an outspoken hedge fund manager, questioned whether private-equity
firms “are appropriating profits that should belong to public shareholders.”
With profit opportunities so rich, Wall Street firms are getting into the
business themselves. Merrill Lynch, which had acted as a longtime adviser to
HCA, switched sides to become a buyer after persuading the company to sell
itself. Goldman Sachs has also become heavily involved in the private-equity
business.
Yet while private equity has been known as “fast money” for flipping businesses,
increasingly the firms are looking to hold assets for longer periods. “Now that
private equity has become institutionalized, it has allowed us to have a longer
timeframe,” said Stephen Pagliuca of Bain Capital, one of the buyers of HCA who
added that he might hold the company for more than the typical five years.
Still, it remains possible that the private-equity market could be a bubble, a
fact Mr. Rubenstein of Carlyle Group readily acknowledges. “We may be at the
top, but we won’t know for a few years.”
The Kohlberg Kravis deal for RJR Nabisco — first announced in October 1988 and
then won months later — proved to be the top of the market and a very difficult
deal for the firm, which eked out only a modest profit after years of struggle.
In an odd twist, two of the firms that agreed yesterday to acquire HCA — Bain
and Kohlberg Kravis — had passed on buying HCA in 1988, when it took itself
private. HCA went public again in 1992 — and may very well do so again in a few
years when its private-equity investors look to cash out.
HCA
Buyout Highlights Era of Going Private, NYT, 25.7.2006,http://www.nytimes.com/2006/07/25/business/25buyout.html?hp&ex=1153886400&en=1825fbcb9615f95b&ei=5094&partner=homepage
Hospital Giant HCA Is Close to a Record
Buyout
July 24, 2006
The New York Times
By ANDREW ROSS SORKIN
HCA, the nation’s largest for-profit hospital
operator, was close to a deal last night to sell itself to a consortium of
private equity investors for about $21 billion, people involved in the talks
said. The investors would also take on about $10.6 billion of HCA’s debt, making
the deal the largest leveraged buyout in history.
The buyout group is led by Thomas Frist Sr., the founder of HCA, and his son,
Thomas F. Frist Jr., who are, respectively, the father and brother of Senator
Bill Frist, the majority leader. The other investors are Bain Capital, Kohlberg
Kravis Roberts & Company and Merrill Lynch’s private equity arm, these people
said.
With a value of $31.6 billion the deal would be even larger than Kohlberg Kravis
Roberts’ $25 billion acquisition of RJR Nabisco in 1989. HCA is planning to vote
on the transaction early today and to announce a deal shortly afterwards.
The potential deal for HCA appears to be driven by trends both on Wall Street
and in the health care industry. For one thing, the private equity business — in
which investment companies pool capital from investors in order to buy companies
and then sell them or take them public — is swimming in cash. And it is eager to
invest in a company like HCA, which generates significant revenue and is
perceived, based on its stock price, as being undervalued by investors.
As a public company, HCA, like many other for-profit hospital companies, has
seen its stock perform poorly in recent years as the whole industry has
struggled with increasing amounts of bad debt as more and more people do not pay
their bills because they do not have sufficient health insurance or any
coverage.
Separately, several enormous acquisitions by private equity firms have taken
place recently: last month, a group of investors bought Univision for $12.3
billion; in May, a group of investors bid $22 billion for Kinder Morgan Inc.; in
April, another group agreed to buy General Motors’ GMAC unit for as much as $14
billion.
These super-sized buyouts are being spurred by an infusion of billions of
dollars of cash to private equity funds. Earlier this month, Blackstone Group
said it had lined up $15.6 billion in commitments for its latest buyout vehicle,
forming the world’s largest private equity fund.
HCA was taken private in the late 1980’s by the company’s management, which at
the time thought it was undervalued. The move turned out to be a success, and
HCA went public again a few years later.
The deal would be a huge boon for Wall Street bankers and lawyers who have been
toiling away on the transaction for months. Credit Suisse, Morgan Stanley and
Shearman & Sterling are advising HCA while Merrill, Bank of America Corporation,
Citigroup Inc., J. P. Morgan Chase and Simpson Thacher & Bartlett are financing
and working for the buying group.
HCA is the nation’s largest for-profit hospital chain, with 2005 revenues of
roughly $25 billion. Headquartered in Nashville, Tenn., the company operates
some 180 hospitals and nearly 100 surgery centers. After merging with Columbia
Hospital Corporation in 1994, HCA became the subject of a widespread federal
Medicare fraud invesigation, which it later settled for $1.7 billion. Thomas
Frist Jr., who had left HCA’s management before the fraud charges, eventually
returned as chief executive in 1997. He stepped down as chairman in 2002 and
remains on the company’s board of directors.
Senator Frist’s ties to the company have drawn criticism over the years as he
has been active in the Senate on a variety of health-care inititiaves that have
the potential to affect the large hospital company. Last fall, the Securities
and Exchange Commission began an investigation into his decision to sell stock,
once estimated at more than $10 million, which was held in a trust.
Senator Frist sold the stock in June, just as the price of HCA stock peaked and
shortly before it fell the following month. The sale was disclosed in September,
and Senator Frist has said he is cooperating fully with the investigation. He
has maintained that the timing of the sale was the result of a decision to
divest his holdings in the company.
Under the terms of the deal now under discussion, the investor consortium would
pay about $51 a share, about a 15 percent premium to HCA’s trading price early
last week when word spread that the negotiations had faltered, people involved
in the talks said. In addition, the buyout group would assume $10.6 billion of
HCA’s debt.
The investor consortium is expected to pay about $6 billion in equity and raise
about $15 billion in debt. With the high-yield bond market tightening, however,
raising that amount of debt could be a challenge.
There is also the possibility that another group could emerge with a rival
offer. HCA has included a provision in its deal with the invetsor consortium
that allows it to actively seek a higher offer. Firms like Blackstone Group and
Apollo Group could look to get involved as could rival hospital groups.
Reed Abelson contributed reporting for this article.
Hospital Giant HCA Is Close to a Record Buyout, NYT, 24.7.2006,
http://www.nytimes.com/2006/07/24/business/24hospital.html?hp&ex=1153800000&en=d152186ab717605d&ei=5094&partner=homepage
Indictment of Doctor Tests Drug Marketing
Rules
July 22, 2006
The New York Times
By ALEX BERENSON
At first, Dr. Peter Gleason thought his arrest
was a joke.
In the early afternoon of Monday, March 6,
half a dozen men in suits surrounded Dr. Gleason, a Maryland psychiatrist, at a
train station on Long Island and handcuffed him.
“I said, ‘Well, this is a gag,’ ” Dr. Gleason recalled in a recent interview.
“They said, ‘No, this isn’t.’ ”
Dr. Gleason, 53, was taken aback because he was arrested, and later charged, for
doing something that has become common among doctors: promoting a drug for
purposes other than those approved by the federal government.
But prosecutors say that Dr. Gleason went too far. At hundreds of speeches and
seminars where he was rewarded with generous fees, Dr. Gleason advised other
physicians that a powerful drug for narcolepsy could be prescribed for
depression and pain relief. In doing so, he conspired with the drug’s
manufacturer to recommend it for potentially dangerous uses, the prosecutors
claim.
The case has put the spotlight on the murky financial relationships between drug
companies and the physicians they use to promote their medicines. Companies
cannot directly advertise drugs for purposes not approved by the Food and Drug
Administration. But getting drugs prescribed for unapproved uses can increase a
drug’s sales, so companies often skirt the rules by sponsoring seminars where
doctors are paid to make presentations promoting their drugs, including the “off
label” uses.
For doctors, these and other payments they receive for discussing drugs can be
very lucrative. Dr. Gleason acknowledges that he received more than $100,000
last year alone from Jazz Pharmaceuticals, which makes Xyrem, the narcolepsy
drug he has promoted.
His case could establish limits on what doctors can do to help companies sell
their drugs. But any precedent could be complicated by the history of Xyrem,
which differs in one important way from other drugs. Because the active
ingredient in Xyrem is gamma hydroxybutyrate, or GHB, an illegal street drug
with a history of use in date rape and of overdose hazards, Xyrem is listed as a
federally controlled substance, with distribution tightly monitored.
Some doctors who have researched Xyrem say that Dr. Gleason, in his enthusiasm
for the drug, may have understated its very real risks. Still, at least one
former F.D.A. official says that the government appears to be overreaching in
going after Dr. Gleason and may chill a common and legitimate form of medical
discussion. “This is a very, very scary development,” said Daniel E. Troy, a
partner at Sidley Austin and the former chief counsel of the F.D.A.
Dr. Steven Nissen, the interim chairman of cardiovascular medicine at the
Cleveland Clinic, said the case could “have a chilling effect on physicians,
because when we give lectures, we assume that giving an opinion about the use of
a drug is not going to get us into legal difficulty.” The F.D.A. and federal
lawyers, he said, need to restrict criminal prosecutions to especially egregious
cases of off-label promotion.
Continuing to Practice
Dr. Gleason, who is now free on bail and continues to practice medicine, insists
that he is not guilty of conspiracy. He says that he was charged only after he
refused to help the government build a case against the drug’s maker, Jazz
Pharmaceuticals — a sequence of events that court documents seem to support.
Dr. Gleason freely acknowledges that in meetings with other doctors, he
advocated Xyrem as a treatment for many conditions, including depression and
fibromyalgia, a poorly understood pain disorder.
In a news release about the indictment, an assistant F.B.I. director compared
Dr. Gleason to a “carnival snake-oil salesman.”
But the doctor says that based on his own experience giving Xyrem to patients,
he believes everything he said about the drug and that his right to express his
views are protected by both F.D.A. rules and the First Amendment.
Some lawyers who have reviewed Dr. Gleason’s case, but are not representing him,
say they agree.
Dr. Gleason has been trapped in the complex rules that cover what doctors and
drug manufacturers are allowed to say about prescription drugs, according to
Harvey A. Silverglate, a lawyer in Boston who specializes in civil liberties
cases.
“What they are doing is criminalizing conduct that is not clearly criminal,”
said Mr. Silverglate, who is not involved in Dr. Gleason’s defense.
Neither the F.D.A. nor the United States attorney’s office in Brooklyn, which
indicted Dr. Gleason, would comment on the case. Nor would David Loftus, a
public defender who took over the case after Dr. Gleason determined he could not
afford a private lawyer. Jazz Pharmaceuticals, which has not been charged, also
declined to comment.
F.D.A. rules allow doctors to prescribe federally approved drugs for any
purpose, even if it is not indicated on the medicine’s label. But drug companies
are tightly constrained in what they can say about their medicines. Companies
can promote drugs only for their federally approved purposes — their so-called
“on label” use.
“Off label” promotion by drug companies is illegal, and since 2000 drug makers
have paid large fines to settle federal criminal cases over off-label
prescriptions.
Pfizer, for example, paid $430 million in 2004 to settle allegations that it had
promoted Neurontin, an anti-epilepsy medicine, for pain and bipolar disorder.
Despite the F.D.A.’s constraints on drug makers, though, the companies are
allowed to hire independent doctors to talk to other physicians about their
medicines. Companies can also sponsor “continuing medical education” sessions,
ranging from lunches to weeklong conferences, where specialist doctors tell
other physicians about the latest developments in their fields — including
off-label uses for drugs already on the market. For such speaking engagements,
doctors can receive $3,000 or more a day from the companies.
In other words, the F.D.A. rules allow drug makers to pay independent doctors to
discuss medicines in ways that might be illegal for the companies themselves.
Beyond the federal rules, guidelines by doctors’ groups give physicians wide
latitude to talk about off-label use.
The American Medical Association considers continuing-education sessions
valuable and believes that doctors should be free to prescribe drugs for
off-label use, according to Dr. Edward Langston, a member of the A.M.A. board.
In general, though, he said, the A.M.A. believes doctors should rely on
peer-reviewed research, not anecdotal evidence, when they write off-label
prescriptions.
The Accreditation Council for Continuing Medical Education, which oversees the
groups that create medical education sessions, loosened its rules in 2004 so
that speakers would not have to disclose whether a recommended use is on-label
or off-label, said Dr. Murray Kopelow, the council’s chief executive.
“The A.C.C.M.E. abandoned the distinction between off-label and on-label,’’ Dr.
Kopelow said. Instead speakers should make recommendations based on accepted
medical and scientific evidence, he added.
Dr. Gleason acknowledges that he did not follow those evidence-based guidelines
when discussing Xyrem in hundreds of speeches and seminars from 2003 to 2006.
The talks were paid for by the original maker of Xyrem, a company called Orphan
Medical. Orphan was acquired by Jazz Pharmaceuticals in June 2005.
In one seminar cited in the federal indictment, a session last August in Denver,
Dr. Gleason told doctors that “table salt is more dangerous” than Xyrem — a
statement scoffed at by other experts on the drug.
An Aid to Sleep Quality
Xyrem’s active ingredient GHB is a fast-acting central nervous system depressant
developed as an anesthetic in the 1960’s. The drug improves sleep quality,
enabling narcoleptics to stay awake the next day, according to physicians who
specialize in treating sleep disorders. But because GHB can suppress breathing,
overdoses can cause coma or death.
“It has the potential to do a lot of good if it’s used properly, the potential
to do a lot of harm if it’s used improperly,” said Dr. Martin Scharf, the
director of the Tri-State Sleep Disorders Clinic in Cincinnati, who said he had
studied GHB in hundreds of patients since the early 1980’s.
In 2000, after highly publicized cases in which young women died or were raped
after GHB was slipped into their drinks, Congress designated the drug a Schedule
I controlled substance, in the same class as heroin.
But by then, doctors had shown that GHB could treat cataplexy, a variant of
narcolepsy that causes people to suffer temporary paralysis. After lobbying from
doctors and Orphan Medical, Congress said that if the F.D.A. chose to approve
prescription GHB, it would be designated as a Schedule III controlled substance,
legal for medical use, like the painkiller Vicodin or steroids.
In 2002, after Orphan presented clinical trial data showing GHB’s effectiveness
against cataplexy, the F.D.A. approved the drug, under the brand name Xyrem, as
a cataplexy treatment. In 2005, the agency approved Xyrem for the treatment of
all forms of narcolepsy.
To help persuade the F.D.A. to approve Xyrem, Orphan Medical agreed to make the
drug available only from a single pharmacy in Missouri, which ships it to
patients nationally. No other prescription drug, even other Schedule III
medicines, is so tightly controlled. For now, Xyrem, which costs more than $600
a month, is a niche product, with sales of about $25 million last year.
Dr. Gleason said he had been interested in Xyrem even before the drug was
officially approved because he believed that other medicines for insomnia and
depression were addictive or had serious side effects. “I immediately just
started prescribing this stuff in 2002,” he said.
He prescribed the drug to about 100 of the patients he saw in his private
practice in Maryland, almost always for off-label conditions like insomnia and
severe depression. Xyrem seemed to work better than existing treatments, he
said.
By early 2003, a sales representative for Orphan Medical, noting Dr. Gleason’s
high rate of prescriptions, asked him if he would give talks to other doctors
about Xyrem.
“I started doing those, and I started getting requested a lot,” Dr. Gleason
said. He received $450 to visit a doctor in the office, $750 for speaking at a
luncheon and $1,500 for a dinner speech. He made as much as $3,000 a day, he
said.
Although he continued to see some patients, the Xyrem talks gradually became his
primary source of income.
In April 2005, after a tip from a whistleblower inside Orphan Medical, the
government began investigating Dr. Gleason and the company, according to an
affidavit that Darren Petri, a criminal investigator for the F.D.A., filed in
February in support of an arrest warrant for Dr. Gleason.
The affidavit says that a cooperating witness repeatedly taped Dr. Gleason as he
discussed Xyrem, including the Denver talk where he compared Xyrem to table salt
and a meeting in November where he said Xyrem was safe for children.
The indictment also charges that Dr. Gleason committed fraud against insurance
companies by advising doctors to leave blank an area on the Xyrem prescription
form that asked for a disease diagnosis. Dr. Gleason acknowledges that he told
doctors not to offer a diagnosis but says he never told them to lie if they were
asked for one.
Dr. Gleason says he did not know he was under investigation when he went to
Great Neck, N.Y., on March 5 to talk to doctors about Xyrem during a lunch
meeting at the office of Dr. Richard Blanck, a neurologist. The meeting had been
arranged by a Jazz Pharmaceuticals salesman, Al Caronia, Dr. Gleason said.
An Unexpected Arrest
Dr. Blanck confirmed the meeting and said Dr. Gleason’s comments seemed typical
for a sales presentation sponsored by a drug company. Mr. Caronia did not return
calls seeking comment.
Afterward, Dr. Gleason says that Mr. Caronia drove him to the Long Island Rail
Road station in the village center, to begin his journey home. When he stepped
out of the car, Dr. Gleason says, Mr. Petri and other investigators surrounded
him, bundled him into a sport utility vehicle and drove him to the Great Neck
police station.
Mr. Caronia was not arrested.
The federal agents said he would have to cooperate in their investigation into
Jazz Pharmaceuticals, Dr. Gleason contends. “They said, ‘Who in this company
roped you into this conspiracy?’ ’’
Insisting that he had broken no laws, Dr. Gleason said he tried to persuade Mr.
Petri and the others that his views on Xyrem were scientifically based. He was
released later that day.
Dr. Gleason’s account is at least partly supported by a letter on March 13 from
Geoffrey Kaiser, an assistant United States attorney, to Lois Bloom, the federal
magistrate judge overseeing the case. In the letter, Mr. Kaiser asks that the
case be kept quiet because Mr. Gleason may “be willing to cooperate with this
office in its broader investigation.”
On Bail and Short on Work
The same day, Dr. Gleason was arraigned in Federal District Court in Brooklyn,
where he was released on a $150,000 bond.
It was not until three weeks later, on April 5, that the federal attorney’s
office announced Dr. Gleason’s arrest, with the news release comparing him to a
snake-oil salesman. As he awaits further hearings and trial, Dr. Gleason, who is
divorced, is supporting himself by working as an in-house doctor on short-term
contracts. For a brief period, he worked at a Maryland state hospital, before
being let go. He said the hospital told him he had been fired because of the
indictment; a spokesman for the hospital declined to comment.
Now he is filling in at various hospitals in Western states, which he did not
want to identify for fear of losing the work.
As for his former benefactor, Jazz, Dr. Gleason says the company told him it was
now cooperating with the investigation and that he would have to face the
indictment on his own.
“They’re just cutting me loose,” he said.
For all that, Dr. Gleason said he still believed in Xyrem. “The only thing
symmetrical with the efficacy and safety of GHB is the hysteria about it.”
Those sorts of claims discomfort even other doctors and researchers who agree
that the drug may be useful.
“He is a very smart man, and I believe he is extremely well intentioned,” Dr.
Scharf said. “But this is not candy. It’s not a cure-all.”
Indictment of Doctor Tests Drug Marketing Rules, NYT, 22.7.2006,
http://www.nytimes.com/2006/07/22/business/22drugdoc.html?hp&ex=1153627200&en=c30b0a9f04a0d5c0&ei=5094&partner=homepage
Schwarzenegger gives $150M stem cell loan
Updated 7/22/2006 1:49 PM ET
AP
USA Today
SACRAMENTO (AP) — A day after President Bush
vetoed expanded federal funding of embryonic stem cell research, Gov. Arnold
Schwarzenegger on Thursday authorized a $150 million loan to fund California's
stem cell institute, which has been stalled by lawsuits.
Schwarzenegger, a Republican who has been
trying to put distance between himself and the unpopular president as he seeks
re-election this year, said the state cannot afford to wait to fund the science
associated with stem cells.
"I remain committed to advancing stem cell research in California, in the
promise it holds for millions of our citizens who suffer from chronic diseases
and injuries that could be helped as a result of stem cell research,"
Schwarzenegger said in a letter to his finance director.
The state's voters created the California Institute for Regenerative Medicine in
2004 when they passed a ballot measure that authorized $3 billion over 10 years
for stem cell research.
Lawyers with ties to anti-abortion and anti-tax groups have sued, arguing that
the institute is unconstitutional.
On April 21, a Superior Court judge ruled the institute was a legitimate state
agency. But if opponents continue to contest the agency in court, they could
hold up the institute's financing until at least next year.
Elsewhere, Illinois Gov. Rod Blagojevich, a Democrat, announced Thursday that he
is diverting $5 million from the state budget for stem cell research, despite
repeated objections from state legislators.
"Investing in research that can save lives and prevent serious illnesses is more
than a sound public health strategy, it's our moral obligation," he said.
The money will come out of administrative funds already set aside for the state
Department of health care and Family Services, Blagojevich said.
Last year Blagojevich used an executive order to spend $10 million for stem cell
research, a move that caught many state lawmakers off guard. Illinois lawmakers
have previously voted against stem cell research, and this spring they did not
take up the governor's proposal for $100 million in funding over five years.
Legislators of both political parties criticized his move Thursday.
"Any time this happens, it's not good for the process when you circumvent the
legislative body and the voice of the people," said Democratic Rep. John
Bradley.
Embryonic stem cells are building blocks that turn into different types of
tissue. Scientists hope to use them someday to regenerate damaged organs or
other body parts and cure diseases. Some oppose such research because it entails
the destruction of human embryos.
Schwarzenegger gives $150M stem cell loan, UT, 22.7.2006,
http://www.usatoday.com/news/nation/2006-07-22-california-stem-cells_x.htm
Jimmy Margulies
New Jersey -- The Record Cagle
20.7.2006
http://cagle.msnbc.com/politicalcartoons/PCcartoons/margulies.asp
First Bush Veto Maintains Limits on Stem
Cell Use
July 20, 2006
The New York Times
By SHERYL GAY STOLBERG
WASHINGTON, July 19 — President Bush on
Wednesday rejected legislation to expand federally supported embryonic stem cell
research, exercising his first veto while putting himself at odds with many
members of his own party and what polls say is a majority of the public.
By defying the Republican-controlled Congress, which had sent him legislation
that would have overturned research restrictions he imposed five years ago, Mr.
Bush re-inserted himself forcefully into a moral, scientific and political
debate in which Republicans are increasingly finding common ground with
Democrats.
The president laid out his reasoning in a written message to the House of
Representatives, then announced his decision in the East Room of the White
House, surrounded by babies born through in vitro fertilization using so-called
“adopted embryos.’’
As the infants gurgled and fidgeted in their parents’ arms, Mr. Bush said the
bill violated his principles on the sanctity of human life by encouraging the
destruction of embryos left over from fertilization procedures. Proponents of
the measure have argued that such embryos would be destroyed anyway.
“I felt like crossing this line would be a mistake, and once crossed we would
find it almost impossible to turn back,’’ Mr. Bush said. “Crossing the line
would needlessly encourage a conflict between science and ethics that can only
do damage to both, and to our nation as a whole.’’
Until Wednesday, Mr. Bush was among just seven presidents — all of whom served
before 1881 — who had never vetoed a piece of legislation. Four served only
partial terms; the other three were John Adams, Thomas Jefferson and John Quincy
Adams.
Within hours of the East Room ceremony, the House hurriedly took up a measure to
override the veto, but the vote, 235 to 193, fell 51 short of the two-thirds
majority required. Fifty-one Republicans, 183 Democrats and 1 independent voted
to override, while 4 Democrats joined 179 Republicans in voting to keep the veto
intact.
The vote put an end to the bill’s prospects for the year, but not to the stem
cell debate, which has escalated into a major issue on Capitol Hill, with
Democrats and Republicans alike predicting electoral repercussions in November.
“This is not some wedge issue; this is the soul of America,’’ said
Representative Diana DeGette, Democrat of Colorado, who sponsored the bill Mr.
Bush vetoed. “And this is a colossal mistake on the part of the president.’’
But beyond the principles involved, the White House had clearly calculated that
it would have been more of a political mistake to sign the bill. Social
conservatives, the heart of Mr. Bush’s base, had demanded the president keep his
promise to veto any measure that altered the careful compromise he articulated
in 2001. With Mr. Bush’s approval ratings hovering at about 40 percent,
conservatives are more critical than ever to the president, and he cannot afford
to arouse their ire.
“This is a profound moral issue,’’ said Representative Mike Pence, Republican of
Indiana, after the White House ceremony. “The issue is whether or not it is
morally right to use the taxpayer dollars of millions of pro-life Americans who
find this research morally objectionable.’’
Yet the ground is shifting in the debate, and even Mr. Pence conceded that
opponents of the research were ‘’losing the argument with the American people.’’
Republicans, even those like Mr. Bush who oppose abortion, are wrestling with
whether embryos that are no bigger than a typographical period but regarded by
some as human beings should be destroyed to save lives.
The issue reflects the complex nature of the politics of abortion and medical
research in the United States today and is in some ways the flip side of the
Democrats’ quandary over abortion. Just as medical advances like ultrasound
imaging have spurred greater opposition to abortion, leading some Democrats to
recalibrate their views, the promise of embryonic stem cell research has pushed
some Republicans toward positions in which black-and-white beliefs about the
sanctity of life have given way to more nuanced and ethically complex stances.
As baby boomers have aged, demanding the best medical treatments for themselves
and their elderly parents, the public clamor for stem cell research has grown
more intense. According to the Pew Research Center, a nonpartisan polling
organization that tracks the issue, roughly two-thirds of all Democrats and
independents favor embryonic stem cell research, while nearly half of all
Republicans do.
That leaves Mr. Bush — who has not used his veto partly because Republicans have
controlled both houses of Congress for nearly all of his presidency — at odds
with many leaders of his own party. They include staunch abortion opponents like
Senators Orrin G. Hatch of Utah, Gordon H. Smith of Oregon and the Senate
majority leader, Bill Frist of Tennessee. Already, some Republicans who opposed
Mr. Bush on the stem cell issue are looking to the presidential elections of
2008.
“When there’s another election, another chapter of democracy opens,’’ Mr. Smith
said in an interview. “Most of the candidates who have a shot at winning are in
favor of stem cell research. This represents a delay en route, but I know where
we’re going, and it’s where the American people want to go.’’
As the White House prepared for the East Room ceremony, advocates for patients
who support stem cell research flooded the switchboard with calls urging Mr.
Bush not to veto the bill.
“We were really hoping, because so many of the American people supported this
research, that the president would take this opportunity to take a really big
deep breath and reconsider,” said Kathy Lewis, president of the Christopher
Reeve Paralysis Foundation, named for the late actor who was an outspoken
advocate for the science.
In a sense, the issue has come full circle for Mr. Bush. The president devoted
his first prime-time television address to the issue, becoming the first
president to open the door to federal financing for the science.
Under the policy, which Mr. Bush announced on Aug. 9, 2001, the federal
government pays for studies on stem cell colonies, or lines, created before that
date, so that the government does not encourage the destruction of additional
embryos. Mr. Bush said Wednesday that his administration had made more than $90
million available for such work.
The bill Mr. Bush vetoed would have allowed taxpayer-financed research on lines
derived from embryos slated for destruction by fertility clinics. Mr. Bush also
signed a “fetal farming” measure, barring trafficking in embryos and fetuses
with the intent of harvesting body parts.
“These boys and girls are not spare parts,” the president said in a speech that
was interrupted repeatedly by hoots of applause, and twice by standing ovations.
“They remind us of what is lost when embryos are destroyed in the name of
research.’’
In one respect, the veto plays to Mr. Bush’s personal strengths, reinforcing the
perception that he is someone who makes up his mind and sticks to it, ignoring
the polls. But Democrats are determined to make the veto a central theme of
their fall election campaigns, hooking it in with another hugely divisive
medical issue — the Terri Schiavo right-to-die case — to argue that Republicans
are beholden to the religious right.
Within hours of the veto, the Senate Democratic leader, Harry Reid of Nevada,
sent out a fund-raising letter asserting that Mr. Bush had decided that curing
diseases “was not as important as catering to his right-wing base.”
Representative Edward J. Markey, Democrat of Massachusetts, put it this way:
“This will be remembered as a Luddite moment in American history.”
Even Republicans concede the president’s action could hurt their candidates,
particularly moderates like Representative Christopher Shays of Connecticut, who
face tough re-election contests.
“It paints us in a corner as more and more single issue, and more and more
unreasonable,” said Ed Rollins, a Republican strategist. “This is the line that
the president certainly doesn’t want Republicans to cross, but I think an awful
lot of Republicans say this goes across common sense, this research has the
potential of saving my father, my mother, or a friend, or curing cancer.”
First
Bush Veto Maintains Limits on Stem Cell Use, NYT, 20.7.2006,
http://www.nytimes.com/2006/07/20/washington/20bush.html?hp&ex=1153454400&en=5bd39aa1c9072bd1&ei=5094&partner=homepage
Just Another Face in the Crowd,
Indistinguishable Even if It’s Your Own
July 18, 2006
The New York Times
By NICHOLAS BAKALAR
Some people never forget a face. Heather
Sellers never remembers one.
She finds it almost impossible to recognize people simply by looking at them.
She remembers the books she reads as well as anyone else, but movies and TV
shows are impossible to follow because all of the actors’ faces seem so similar.
She can recall a name or a telephone number with ease, but she is unable to
remember her own face well enough to pick it out in a group photograph.
Dr. Sellers, a professor of English at Hope College in Holland, Mich., has a
disorder called prosopagnosia, or face blindness, and she has had it since
birth. “I see faces that are human,” she said, “but they all look more or less
the same. It’s like looking at a bunch of golden retrievers: some may seem a
little older or smaller or bigger, but essentially they all look alike.”
Face blindness can be a rare result of a stroke or a brain injury, but a study
published in the July issue of The American Journal of Medical Genetics Part A
is the first report of the prevalence of a congenital or developmental form of
the disorder.
The researchers say the phenomenon is much more common than previously believed:
they found that 2.47 percent of 689 randomly selected students in Münster,
Germany, had the disorder.
Dr. Thomas Grüter, a co-author of the paper, said there were reasons to believe
that the condition was equally common in other populations. “First,” he said,
“our population was not selected in terms of cognition deficits. And second, a
study done by Harvard University with a different diagnostic approach yielded
very similar figures.”
Dr. Grüter is himself prosopagnosic. His wife and co-author, Dr. Martina Grüter
of the Institute for Human Genetics at the University of Münster, did not
realize he was face blind until she had known him more than 20 years. The
reason, she says, is he was so good at compensating for his deficits.
“How do you recognize a face?” she asked. “For most people, this is a silly
question. You just do. But people who have prosopagnosia can tell you exactly
why they recognize a person. Thomas consciously looks for the details that
others notice unconsciously.”
Dr. Thomas Grüter’s experience in this respect is typical of people with face
blindness. They develop alternate strategies for identifying people — they
remember their clothes, mannerisms, gait, hairstyle or voice, and by using such
techniques, many can compensate quite well.
This may be one reason why cases of prosopagnosia have so rarely been reported —
people simply do not know they have it. For face-blind people, adaptations like
these are the only choice; there is no known cure.
“Until very recently, not remembering faces was not considered to be a medical
condition,” Dr. Thomas Grüter said. “It was not even known to most physicians as
such. The term ‘prosopagnosia’ was not taught to students of medicine or
psychology.” Most people “would consider it a bad habit,” he said, “much like
forgetting the names of people you are introduced to, or being unable to find
your way around town.”
Dr. Martina Grüter said many considered her husband and his father, who is also
face blind, to be simply “absent-minded professors” who occasionally may not
recognize someone because they are preoccupied with higher thoughts.
People with face blindness can typically understand facially expressed emotions
— they know whether a face is happy or sad, angry or puzzled. They can detect
subtle facial cues, determine gender and even agree with everyone else about
which faces are attractive and which are not. In other words, they see the face
clearly, they just do not know whose face they are looking at, and cannot
remember it once they stop looking.
Even familiar faces can be unrecognizable. Dr. Sellers, for example, said she
could summon no picture in her mind of her own mother’s face.
Dr. Sellers discovered her own problem only a year ago, at the age of 40. She
was doing research for a novel involving a character with schizophrenia. “I kept
coming across the term ‘face recognition,’ ” she said. “It kept ringing a bell,
although the phenomenon is quite different for people with schizophrenia. But
once I had the term, I searched for it on the Internet. The minute I knew the
concept of face blindness existed, I knew I had it.”
The phenomenon has been investigated with functional MRI brain scans, a form of
imaging that shows in real time which parts of the brain are active, and it is
known that a part of the brain called the fusiform gyrus responds much more
strongly to faces than to other objects.
Researchers have detected differing responses in this part of the brain among
people with face blindness compared with normal subjects.
“If you show a normal person two different faces in a row,” said Bradley
Duchaine, a lecturer in psychology at University College London, “their brain
response is different with each one. With some prosopagnosics, you don’t see
this different response. It looks like something is not working in those areas
of the brain involved with faces.”
Dr. Duchaine and Ken Nakayama, a psychology professor at Harvard, published a
review of developmental prosopagnosia in the April issue of Current Opinion in
Neurobiology. They run a Web site devoted to the disorder (www.faceblind.org).
Face blindness differs from pervasive cognitive disorders like autism because it
usually involves only one specific symptom. Still, face blindness is sometimes
accompanied by other problems, especially difficulty in finding one’s way around
or, for example, distinguishing one car or dog from another.
Although the specific gene for the disorder has not been found, evidence is
mounting that the trait is inherited. “All pedigrees that we’ve been able to
establish so far were compatible with autosomal dominant inheritance,” Dr.
Thomas Grüter said.
If this turns out to be true, it means that everyone with the disorder will have
at least one affected parent, that men and women will be equally likely to
inherit the trait, and that the risk for each child of an affected parent will
be one in two.
“But we haven’t found the gene, yet,” Dr. Grüter said, “so we can’t be 100
percent sure.”
Just
Another Face in the Crowd, Indistinguishable Even if It’s Your Own, NYT,
18.7.2006,
http://www.nytimes.com/2006/07/18/health/psychology/18face.html?ex=1153454400&en=6c7782d3879488df&ei=5087%0A
Editorial
Standing Up for Stem Cell Research
July 18, 2006
The New York Times
The Senate is poised to vote today on a bill
that would greatly expand the number of embryonic stem cell lines that can be
used in federally financed medical research. This is actually an extremely
modest proposal that would allow the new stem cell lines to be derived only from
surplus embryos otherwise slated for destruction at fertility clinics. Passage
of this bill, which has already been approved by the House, is the very least
the Senate should do to spur advancement of one of the most promising fields of
biomedical research. A two-thirds majority of each house will be needed to
overcome a likely veto from President Bush.
Under current administration policy, scientists can use federal money for
research only on some 22 stem cell lines that already existed when President
Bush announced his policy in August 2001. Those lines were extracted from
microscopic embryos, no bigger than the period at the end of this sentence, that
were inevitably destroyed in the process. Mr. Bush was willing to accept that
fait accompli in the interest of advancing science but said he did not want to
encourage any further destruction of embryos by financing research on additional
lines.
That stance has increasingly hobbled embryonic stem cell research because many
of the existing lines are deteriorating, contaminated or suffer from technical
problems that limit their usefulness. The new proposal would make thousands of
surplus embryos from fertility clinics available for federally funded research,
a change that would be welcomed by most Americans but is opposed by a minority
of religious conservatives.
Our concern with the bill is how limited its reach would be. It would not allow
federal financing of the most promising field of research, known as therapeutic
or research cloning. Therapeutic cloning involves the creation of embryos
genetically matched to patients with specific diseases so that scientists can
extract their stem cells and then study how the diseases develop and how best to
treat them. The microscopic entities used in these studies may be called embryos
but they have none of the attributes of humanity and, sitting outside the womb,
no chance of developing into babies. It is no more immoral to create and destroy
embryos for therapeutic purposes than to create and destroy surplus embryos for
fertility purposes.
But for now the best hope lies with passage of the bill merely allowing use of
surplus fertility clinic embryos. If it passes in the Senate, it seems almost
certain to draw a veto from Mr. Bush, his first in six years in office. Then it
will be up to the House and the Senate to summon the will to override the veto.
If they fail to push through this very limited change in federal policy, voters
will need to hold all recalcitrant legislators accountable for slowing research
that holds great medical potential.
Standing Up for Stem Cell Research, NYT, 18.7.2006,
http://www.nytimes.com/2006/07/18/opinion/18tue1.html
FACTBOX-Stem cells offer therapeutic
promise
Mon Jul 17, 2006 5:11 PM ET
Reuters
(Reuters) - The U.S. Senate is expected to
pass three stem cell bills on Tuesday, including one that would broaden federal
funding of embryonic stem cell research.
Following are some facts about stem cells.
* Stem cells are the body's master cells, the source of all cells and tissue,
such as brain, blood, heart, bones, muscles and skin.
* Embryonic stem cells come from days-old embryos and can produce virtually any
other type of cell in the body. The very earliest embryonic stem cells, up to
five days old, can each give rise to an entire organism.
* Adult stem cells are harbored in mature tissue -- in the bodies of children as
well as adults. They are more specialized than embryonic cells and give rise to
specific cell types, although they may be coaxed into a broader range of cell
types under the right conditions.
* Scientists generally harvest embryonic stem cells from embryos left over after
in-vitro fertilization attempts at fertility clinics. These "test-tube baby"
techniques, used to help infertile couples have a baby, involve fertilizing a
woman's egg cells with a man's sperm cells in a laboratory dish.
Several embryos are created at a time, and not all are implanted into the
mother's womb to create live births. Embryos left over are usually discarded by
the fertility clinic. These can serve as a source of stem cells, a process that
involves removing the blastocyst's inner cells and destroying the embryo.
* Scientists hope to harness the transformational qualities of stem cells to
provide treatments for a variety of diseases affecting millions of people
worldwide. Because stem cells can turn into many other cell types with the right
prompting, doctors may be able to replace tissues and organs damaged by disease
or injury to restore healthy function.
For example, in people with Parkinson's disease, injecting stem cells into the
area of the brain that controls muscle movement, where the disease kills nerve
cells, might regenerate the neurons.
* They also hope to use stem cells to understand the biology of diseases
including cancer and genetic disorders.
* The issue is controversial because some people believe the destruction of any
embryo is wrong. Leaders of the Roman Catholic Church and some other religious
and conservative political figures hold this view, although some opponents of
abortion rights support embryonic stem cell research.
Opponents of embryonic stem cell research believe adult stem cell research
should be pursued instead.
FACTBOX-Stem cells offer therapeutic promise, R, 17.7.2006,
http://today.reuters.com/news/newsArticle.aspx?type=newsOne&storyid=2006-07-17T211021Z_01_N17298752_RTRUKOT_0_TEXT0.xml&WTmodLoc=NewsArt-L1-RelatedNews-1
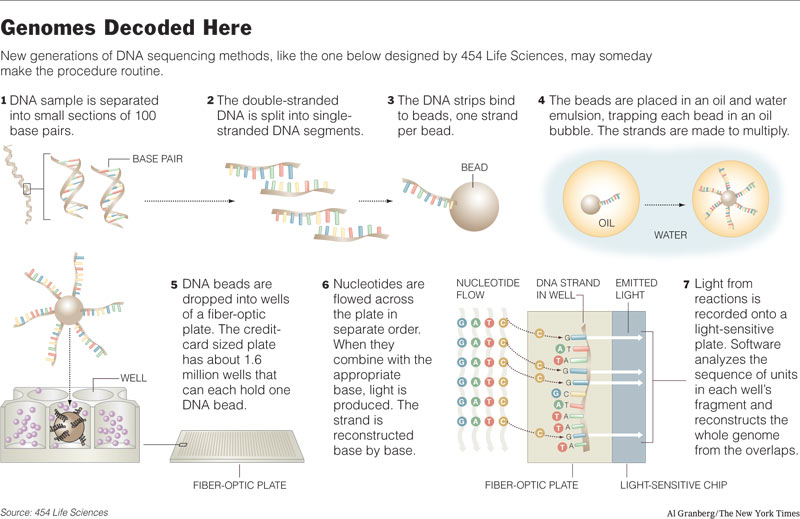
The Quest for the $1,000 Human Genome
NYT 18.7.2006
http://www.nytimes.com/2006/07/18/science/18dna.htm
The Quest for the $1,000 Human
Genome
July 18, 2006
The New York Times
By NICHOLAS WADE
As part of an intensive effort to develop a
new generation of machines that will sequence DNA at a vastly reduced cost,
scientists are decoding a new human genome — that of James D. Watson, the
co-discoverer of the structure of DNA and the first director of the National
Institutes of Health’s human genome project.
Decoding a person’s genome is at present far too costly to be a feasible medical
procedure. But the goal now being pursued by the N.I.H. and by several
manufacturers, including the company decoding Dr. Watson’s DNA, is to drive the
costs of decoding a human genome down to as little as $1,000. At that price, it
could be worth decoding people’s genomes in certain medical situations and, one
day, even routinely at birth.
Low-cost decoding may bring the genomic age to the doctor’s office, but it will
also raise quandaries about how to safeguard and interpret such a wealth of
delicate and far-reaching personal information.
The first human genome decoding, completed by a public consortium of
universities in 2003, cost more than $500 million. With the same technology,
dependent on DNA sequencing machines made by Applied Biosystems, a human genome
could probably now be decoded for $10 million to $15 million, experts say.
Much greater efficiency is expected from the new generation of DNA sequencing
machines, based on different, highly miniaturized technologies. One machine,
made by 454 Life Sciences, has been on the market since March 2005. Another,
made by Solexa, will start shipping this summer. Applied Biosystems will start
marketing its own next-generation machine next year.
Last month, at a training course organized by the Cold Spring Harbor Laboratory
on Long Island, researchers were learning how to use the DNA decoding machines
made by 454 Life Sciences. Looking like a hybrid between a washing machine and a
giant iPod, the machines cost $500,000 each, not counting the computer software
needed to analyze the results.
At their heart lies a plate of light-sensitive chips, the same as those used in
telescopes for detecting faint light from distant stars. On top of the plate
sits a glass slide pitted with thousands of tiny wells, each containing a
fragment of the DNA to be decoded.
As each unit of DNA is analyzed in a well, a flash of light is generated by
luciferase, the enzyme that fireflies use to make themselves glow. The telescope
plate records the twinkling lights from each well and, at the end of the run,
which lasts four or five hours, the sequence of units in each well’s DNA
fragment has been recorded. The fragments are about 100 units in length, and
from their overlaps a computer can then be set to piece together the entire
genome they come from.
In the training course, the project was to analyze DNA from a Tasmanian devil, a
marsupial afflicted with a mysterious malady called devil facial tumor disease.
The researchers found that the genome was laden with a virus that had integrated
its sequence into the devil’s DNA.
The 454 machine can assemble small genomes like those of bacteria, which perhaps
accounted for the presence at the course of three scientists from the Department
of Homeland Security. But the human genome is about 600 times larger than a
bacterium’s and includes many repetitive sequences that, like identical pieces
in a jigsaw puzzle, make the solution much harder.
At the Cold Spring Harbor course, researchers heard Dr. Watson, the laboratory’s
chancellor, say that 454 Life Sciences had asked to sequence his genome with
their new machine. Only two human genomes have been sequenced to date. The
genome sequenced by the public consortium was a mosaic of DNA from several
anonymous people. The consortium’s rival, Celera Genomics, prepared a draft
sequence, most of it from the genome of its former president, Dr. J. Craig
Venter.
Dr. Watson told the students that he had given the company permission to publish
the sequence of his genome, “provided they didn’t release to the world that I
have some disease I don’t want to know about.”
Genomic information can already reveal a lot and will reveal much more as the
roles of new genes are discovered.
“I think that personal genetic information should ordinarily be kept secret,”
Dr. Watson said. “But I have said that 454 can put mine out there, even though
it’s saying something about my sons.”
So far, however, 454 Life Sciences has not published Dr. Watson’s genome, and it
is not clear how much progress the company has made. Christopher K. McLeod, its
chief executive, said, “Technically, we’ve done a lot of good work on it.” But,
he added, “I don’t think we want to discuss where we are.”
Mr. McLeod expressed reservations about releasing personal genetic information,
despite having Dr. Watson’s permission to do so. “Jim feels there are certain
things he’d be comfortable releasing,” he said. “I’m not sure we would agree.”
Another factor may be that the company is developing a more powerful model of
its machine that will be able to read DNA fragments that are 200 or even 400
units in length. These longer-read lengths should make it more feasible to
decode large genomes, like those of people.
The 454 machine is at present being bought chiefly by researchers and by the
large genome sequencing centers established by the public consortium. But it has
begun to show promise for the clinic. One new use is in screening tumors for
genes known to be mutated in cancer, a task that existing machines do not do
well. Spotting which mutation has occurred in a patient’s tumor can help in the
choice of chemotherapy.
Although the 454 model is the only next-generation DNA sequencing machine on the
market, it will be joined this summer by the machine from Solexa. The Solexa
instrument, which will cost $400,000, works on somewhat similar principles but
uses fluorescent dyes to visualize the structure of DNA. And next year Applied
Biosystems will introduce its next-generation machine, based on a technology
developed by George Church of Harvard, said Dennis A. Gilbert, the company’s
chief scientific officer.
Each of the manufacturers claims special advantages for its technology, ensuring
that researchers will have a rich choice.
David Bentley, Solexa’s chief scientist, said that the company’s DNA sequencing
machine had already decoded several bacterial genomes and that he was planning
to sequence a human genome — that of an anonymous man from the Yoruba people of
Nigeria. An African genome was chosen because there is greater genetic diversity
in African populations, Dr. Bentley said.
The demand for whole genome sequencing is a long way off, in Dr. Bentley’s view,
but not so distant that it is too early to think about the consequences of
generating such information. He advocates that two people should control access
to a person’s genome sequence — the patient and the physician.
Why not the patient alone? Dr. Bentley said genomes would be so difficult to
analyze correctly that interpretation should stay within the medical profession.
Otherwise, freelance services will spring up, offering to predict whether a
person will get heart disease or their age of death. This potential for
misinformation “would have a huge adverse impact on the medical use of genetic
information,” Dr. Bentley said.
A recent example of genetic misinformation occurred last month when a DNA
testing genealogy company, Oxford Ancestors, told Thomas R. Robinson, an
accountant at the University of Miami, that he was a descendant of Genghis Khan.
Only because Mr. Robinson sought a second opinion did he find that the
information was incorrect.
Technology, not medicine, is the immediate force behind the quest for the $1,000
human genome. The new decoding machines are being developed because they are
possible, not because hospitals are demanding them. But the makers expect that
demand will grow as researchers develop new uses.
“As we drop the price and increase the capability, there are applications that
couldn’t be done before,” like a researcher being able to screen a thousand
patients for cancer mutations, Dr. Gilbert said.
At present, only a handful of genes are monitored by doctors in clinical
practice, and specific tests for these genes make it unnecessary to decode a
person’s entire genome. But at some point, the new machines or their successors
may make genome decoding a routine medical test.
Already, every newborn baby endures its heel being pricked to draw a few drops
of blood, which are tested for a handful of enzymic deficiencies. But when
genomes can be decoded for $1,000, a baby may arrive home like a new computer,
with its complete genetic operating instructions on a DVD.
The
Quest for the $1,000 Human Genome, NYT, 18.7.2006,
http://www.nytimes.com/2006/07/18/science/18dna.html
Paralyzed Man Uses Thoughts to Move a
Cursor
July 13, 2006
The New York Times
By ANDREW POLLACK
A paralyzed man with a small sensor implanted
in his brain was able to control a computer, a television set and a robot using
only his thoughts, scientists reported yesterday.
Those results offer hope that in the future, people with spinal cord injuries,
Lou Gehrig’s disease or other conditions that impair movement may be able to
communicate or better control their world.
“If your brain can do it, we can tap into it,” said John P. Donoghue, a
professor of neuroscience at Brown University who has led development of the
system and was the senior author of a report on it being published in today’s
issue of the journal Nature.
In a variety of experiments, the first person to receive the implant, Matthew
Nagle, moved a cursor, opened e-mail, played a simple video game called Pong and
drew a crude circle on the screen. He could change the channel or volume on a
television set, move a robot arm somewhat, and open and close a prosthetic hand.
Although his cursor control was sometimes wobbly, the basic movements were not
hard to learn.
“I pretty much had that mastered in four days,” Mr. Nagle, 26, said in a
telephone interview from the New England Sinai Hospital and Rehabilitation
Center in Stoughton, Mass. He said the implant did not cause any pain.
Mr. Nagle, a former high school football star in Weymouth, Mass., was paralyzed
below the shoulders after being stabbed in the neck during a melee at a beach in
July 2001. He said he had not been involved in starting the brawl and did not
even know what had sparked it. The man who stabbed him is now serving 10 years
in prison, he said.
Implants like the one he received had previously worked in monkeys. There have
also been some tests of a simpler sensor implant in people, as well as systems
using electrodes outside the scalp. And Mr. Nagle has talked before about his
experience.
But the paper in Nature is the first peer-reviewed publication of an experiment
in people with a more sophisticated implant, able to monitor many more brain
neurons than earlier devices. The paper helps “shift the notion of such
‘implantable neuromotor prosthetics’ from science fiction towards reality,”
Stephen H. Scott, professor of anatomy and cell biology at Queen’s University in
Ontario, wrote in a commentary in the journal.
The sensor measures 4 millimeters by 4 millimeters — less than a fifth of an
inch long and wide — and contains 100 tiny electrodes. The device was implanted
in the area of Mr. Nagle’s motor cortex responsible for arm movement and was
connected to a pedestal that protruded from the top of his skull.
When the device was to be used, technicians plugged a cable connected to a
computer into the pedestal. So Mr. Nagle was directly wired to a computer,
somewhat like a character in the “Matrix” movies.
Mr. Nagle would then imagine moving his arm to hit various targets. The
implanted sensor eavesdropped on the electrical signals emitted by neurons in
his motor cortex as they controlled the imaginary arm movement.
Obstacles must be overcome, though, before brain implants become practical. For
one thing, the electrodes’ ability to detect brain signals begins to deteriorate
after several months, for reasons not fully understood. In addition, the implant
would ideally transmit signals wirelessly out of the brain, doing away with the
permanent hole in the head and the accompanying risk of infection. Further, the
testing involving Mr. Nagle required recalibration of the system each day, a
task that took technicians about half an hour.
Still, scientists said the study was particularly important because it showed
that the neurons in Mr. Nagle’s motor cortex were still active years after they
had last had a role to play in moving his arms.
The implant system, known as the BrainGate, is being developed by Cyberkinetics
Neurotechnology Systems Inc. of Foxborough, Mass. The company is now testing the
system in three other people, who remain anonymous: one with a spinal cord
injury, one with Lou Gehrig’s disease and one who had a brain stem stroke.
Timothy R. Surgenor, president and chief executive, said Cyberkinetics hoped to
have an implant approved for marketing as early as 2008 or 2009. Dr. Donoghue,
the chief developer, is co-founder and chief scientist of Cyberkinetics. Some of
the paper’s other authors work at the company, while still others are from
academic or medical institutions including Massachusetts General Hospital.
Like his performance in other tasks, Mr. Nagle’s control of the computer cursor
was not particularly smooth. When his goal was to guide the cursor from the
center of the screen to a target on the perimeter, he hit the target 73 to 95
percent of the time. When he did, it took 2.5 seconds on average, but sometimes
much longer. And the second patient tested with the implant had worse control
than he, the paper said.
By contrast, healthy people moving the cursor by hand hit the target almost
every time, and in only one second.
Dr. Jonathan R. Wolpaw, a researcher at the New York State Department of Health,
said the BrainGate performance did not appear to be substantially better than
that of a noninvasive system he is developing using electroencephalography, in
which electrodes are placed outside the scalp.
“If you are going to have something implanted into your brain,” Dr. Wolpaw said,
“you’d probably want it to be a lot better.”
Dr. Donoghue and other proponents of the implants say they have the potential to
be a lot better, because they are much closer to the relevant neurons than are
the scalp electrodes, which get signals from millions of neurons all over the
brain.
One way to improve implant performance was suggested by another paper in the
same issue of Nature. In a study involving monkeys, Krishna V. Shenoy and
colleagues at Stanford University eavesdropped not on the neurons controlling
arm movement but on those expressing the intention to move, which occurs earlier
and would make the system work faster.
“Instead of sliding the cursor out to the target, we can just predict which
target would be hit and the cursor simply leaps there,” said Dr. Shenoy, an
assistant professor of electrical engineering and neurosciences. He said the
system could operate at the equivalent of typing 15 words a minute, about four
times as fast as the devices produced by Cyberkinetics and Dr. Wolpaw.
After more than a year, Mr. Nagle had his implant removed so he could undergo
another operation, which allowed him to breathe without a ventilator. He can
control a computer by voice, so he does not really need the implant. But he said
he was happy he had volunteered for the experiment.
“It gave a lot of people hope,” he said.
Paralyzed Man Uses Thoughts to Move a Cursor, NYT, 13.7.2006,
http://www.nytimes.com/2006/07/13/science/13brain.html
F.D.A. Backs AIDS Pill to Be Taken Once a
Day
July 13, 2006
The New York Times
By ANDREW POLLACK
The first drug that allows AIDS to be treated
by taking one pill a day won federal approval yesterday, a development that
government officials said would both simplify and improve treatment of the
disease.
The drug, called Atripla, is a combination of three once-a-day drugs that are
already on the market — Sustiva from Bristol-Myers Squibb, and Viread and
Emtriva from Gilead Sciences.
Only a decade ago, when cocktails of AIDS drugs began to be used, patients
sometimes had to take two dozen or more pills a day.
Atripla, which will be available this week or next, will have a wholesale price
of $1,150 a month, equal to the sum of the prices of its components, James
Loduca, a spokesman for Gilead, said.
Both Gilead and Bristol-Myers will market the drug.
The approval by the Food and Drug Administration yesterday, which was expected,
came well before the October deadline for the agency to act. F.D.A. officials
said they moved quickly because a once-a-day treatment would help people take
their medicines faithfully. That would prevent the AIDS virus from gaining
resistance to the drugs.
“It’s one thing to have medicine available, but it will only be effective when
people can indeed take it as they are supposed to,” Dr. Murray M. Lumpkin, an
F.D.A. deputy commissioner, said at a news conference in Washington. Dr. Lumpkin
said a once-a-day treatment would be particularly important for developing
countries, where access to health care is more limited.
Yet no announcement was made yesterday about when the drug would be available
overseas and for what price. An agreement must first be reached with Merck &
Company, which sells Sustiva, also known as efavirenz, in developing countries
under the name Stocrin.
Jeffrey Sturchio, vice president for external affairs at Merck, said his company
had “reached agreement on all the issues with Gilead.” He said it was now a
matter of formalizing the agreement and then applying for approval in various
countries.
He predicted that Atripla would be available in some poor countries in the next
several months at a price that would be roughly the sum of the heavily
discounted prices at which the component drugs are now sold in those places.
Gilead, based in Foster City, Calif., has become one of the most successful
biotechnology companies, based on its AIDS drugs, which accounted for $1.4
billion of its $2 billion in revenue last year. One of its big sellers is
Truvada, a once-a-day combination of Viread, also known as tenofovir, and
Emtriva, also known as emtricitabine. Truvada is usually taken with another
drug, like Bristol-Myers’s Sustiva.
Yaron Werber, an analyst at Citigroup, which counts Gilead as a client, said
that adding the Bristol-Myers drug into a three-drug combination pill would
allow Gilead to take market share from GlaxoSmithKline, which sells a popular
two-drug combination called Combivir.
“I think the drug will do exceptionally well,” Mr. Werber said of Atripla. “The
drug is now the most convenient on the market and it’s probably also the most
potent.”
F.D.A. Backs AIDS Pill to Be Taken Once a Day, NYT, 13.7.2006,
http://www.nytimes.com/2006/07/13/business/13drug.html
New Medicine for AIDS Is One Pill, Once a
Day
July 9, 2006
The New York Times
By ANDREW POLLACK
The first complete treatment for AIDS that is
taken once a day as a single pill is expected to be available soon.
The pill, which combines three drugs made by two companies, would be a milestone
in improving the simplicity of treatment for the disease, experts say. It should
make it easier for people to take their medicine regularly, which is important
for keeping the virus that causes the disease in check.
Only a decade ago, when cocktails of AIDS drugs were first used, patients often
had to take two or three dozen pills a day, some with food, some without, some
so frequently patients had to get up in the middle of the night. Since then, the
regimens have been whittled down to as few as two pills a day, and now, one.
"Going down to one pill a day is amazing," said Keith Folger of Washington, who
started on 36 pills a day about 11 years ago and expects to switch to the new
pill when it becomes available.
Mr. Folger, who is just leaving a job as director of community mobilization for
the National Association of People With AIDS, said the pill would be
"remarkable, especially for people who are starting on medication for the first
time and are sort of freaked out that they will have to take pills for the rest
of their lives."
The new drug is a combination of drugs already on the market — Sustiva, sold by
Bristol-Myers Squibb, and Truvada, sold by Gilead Sciences. Truvada is a
combination of two Gilead drugs, Viread and Emtriva.
The Food and Drug Administration is expected to approve the new drug as soon as
this week. The agency has until October to act but is expected to do so much
sooner, partly because the government has been encouraging companies to do just
this sort of collaboration to come up with simpler AIDS drugs.
The companies have not revealed the new drug's name or its price, though they
have suggested it will cost roughly the same as Sustiva and Truvada bought
separately, which is about $1,200 a month.
There are already other AIDS pills that combine three drugs. One, made by a
company in India, was recently approved by the F.D.A. for use in developing
countries. But those other three-in-one pills generally contain older drugs and
are taken twice a day.
The drugs in the new pill already constitute the most widely prescribed regimen
in the United States and one of the most effective.
Doctors and securities analysts expect most people now taking Sustiva and
Truvada separately to switch to the new pill.
It is somewhat less certain how many people taking other drug combinations will
switch. Some of them will not because the virus in their bodies is already
resistant to one of the drugs in the new pill or because they cannot tolerate
side effects. Sustiva, also known as efavirenz, can cause unsettlingly vivid
dreams and birth defects.
In addition, the new salmon-colored pill is about 1,500 milligrams, the size of
a large vitamin pill, and some people may find it difficult to swallow.
Going to a single pill could be especially important in poor countries, where
patients have less access to medical care and more people are illiterate or
uneducated. The vast majority of the nearly 40 million people in the world
infected by H.I.V., the virus that causes AIDS, are in developing nations. In
the United States there are about 1.1 million.
Bristol-Myers and Gilead say they will make the new pill available at a sharply
reduced price for developing nations, but details are still being worked out.
They are negotiating with Merck & Company, which sells efavirenz in those
countries under the name stocrin.
A once-daily treatment did not become feasible until a few years ago, with the
development of individual drugs that needed to be taken only once a day.
Still, no one company controlled all the drugs needed for an effective
combination. It is rare for rivals to collaborate, though it has been done.
Merck and Schering-Plough, for instance, have put two of their drugs into a
combination cholesterol treatment called Vytorin.
Executives at Bristol-Myers, discussing in 2003 how to increase sales of
Sustiva, came up with the idea of approaching Gilead, which already had two
once-a-day pills, Viread, also known as tenofovir, and Emtriva, or
emtracitabine. Gilead, based in Foster City, Calif., is now the largest supplier
of H.I.V. drugs.
Talks were given further urgency when the F.D.A. summoned the two companies and
Merck to a meeting in Washington in April 2004. The government was trying to
encourage development of simpler pills as part of the president's plan to
provide antiviral treatments to poor countries. The next month, the three
companies announced their plan.
But carrying it out was not easy. Simply combining the three chemicals produced
a mixture that melted easily.
"We made the first formulation and went out for lunch, and when we came back
from lunch we had glue on our hands," said Reza Oliyai, a Gilead scientist. The
eventual solution was to keep Truvada and Sustiva in separate layers.
It also took about a year to find a formulation that would produce the same
level of the three drugs in a patient's blood as the three drugs taken
separately, which is the main requirement for approval of a combination drug.
Gilead tested five different formulations in healthy volunteers.
The failure of patients to take their drugs faithfully is a major problem,
experts say, because it allows H.I.V. to develop resistance to the drugs.
Still, it is unclear exactly how much better people with H.I.V. will stick to a
once-daily regimen compared with one requiring two pills a day.
Bob Huff, who edits a newsletter on new treatments for the Gay Men's Health
Crisis, a patient advocacy group in New York, said a drug's potency and side
effects were more important to patients than convenience.
Still, he said, "For some people it's just what they need to make treatment
doable." A single pill may also mean a single insurance co-payment, he said,
instead of two or three now that can cost people $100 a month.
Michael Weinstein, president of the AIDS Healthcare Foundation, a Los Angeles
organization that runs clinics in the United States and abroad, said other
problems besides inconvenience — like drug addiction, depression and mental
illness — kept people from sticking to their AIDS drugs.
Still, Mr. Weinstein called the new pill a "high-water mark" for simplicity and
the way it was developed. "To have two companies collaborating — that's going to
be significant for the future if it sets an example."
While other companies are expected to try to develop once-daily treatments, no
other existing drugs can yet be as readily combined, said Dr. Calvin Cohen,
research director for the Community Research Initiative of New England, a
nonprofit organization that does clinical trials of H.I.V. drugs and provides
patient education.
Dr. Cohen, an adviser to Gilead, Bristol-Myers and other drug manufacturers,
said there was already some concern among AIDS experts that having a once-a-day
treatment would make people lose their fear of H.I.V. "We still want people to
respect that prevention of the disease is better than treatment," he said.
New
Medicine for AIDS Is One Pill, Once a Day, NYT, 9.7.2006,
http://www.nytimes.com/2006/07/09/health/09aids.html
New AIDS Pill to Treat People in Poor
Countries
July 6, 2006
The New York Times
By DONALD G. McNEIL Jr.
The Food and Drug Administration has approved
the first 3-in-1 antiretroviral pill for use by the American-sponsored plan for
AIDS treatment, something that the White House's acting global AIDS coordinator
said yesterday should greatly improve treatment for AIDS patients in poor
countries.
Although it is not yet clear how much money it will save, having patients take
only one pill twice a day "should facilitate better therapies and better
adherence," said the coordinator, Dr. Mark R. Dybul.
The agency posted the approval of the drug on its Web site on Friday evening. It
approved the 3-in-1 pill, made by an Indian generic drug company, for patients
in countries helped by the President's Emergency Plan for AIDS Relief.
Under that plan, the United States is now the largest provider of antiretroviral
drugs in the world, paying for treatment for 561,000 patients in Africa, Asia
and the Caribbean.
The Global Fund for AIDS, Malaria and Tuberculosis, the second-largest provider,
pays for about 541,000 patients, Dr. Dybul said, although there is some overlap
in countries where both agencies work. (The United States also pays one-third of
the Global Fund's budget.)
The new pill, made by Aurobindo Pharma of Hyderabad, India, combines three
common first-line drugs, AZT, 3TC and NVP, which are also known as zidovudine,
lamivudine and nevirapine and sold in the United States as Retrovir, Epivir and
Viramune.
Dr. Dybul said he was also pleased that the new pill did not contain D4T, also
known as stavudine and Zerit, which is another common first-line drug, but
somewhat more toxic than the others.
In poor countries, where it is harder to do frequent blood and liver tests,
toxicity can be harder to control.
The plan Dr. Dybul runs, known as Pepfar, was created after President Bush's
announcement in his 2003 State of the Union address that he would spend $15
billion over five years to fight AIDS.
At the time, many Bush administration critics feared the money would be reserved
for expensive American and European brand-name drugs. But, defying those
expectations, the program in May 2004 began buying generics and now pays for 24
generic formulations, including liquid solutions for infants. Also, the major
Western companies dropped their prices for poor countries, sometimes as low as
the prices of generics.
However, rather than subscribing to the World Health Organization's
drug-approval process, the president's program requires separate F.D.A.
approval, which has caused delays, even though the agency created a fast-track
process and waived its large fees.
No one from Aurobindo could be reached for comment yesterday, but the company's
Web site carried an announcement, dated Monday, saying it was "delighted to
share" that its drug had won F.D.A. approval.
The first 3-in-1 antiretroviral pill was triomune, from Cipla, another Indian
generic company. It won World Health Organization approval in 2002 and is used
by nearly 400,000 patients whose drugs are bought by Unicef, Doctors Without
Borders and other donors.
Dr. Yusuf K. Hamied, the company's chairman, said yesterday that he hoped for
F.D.A. approval shortly for several Cipla products, including triomune. "Pepfar
came on us out of the blue," he said. "We were concentrating more on the W.H.O.,
and we were a little slow catching up." Nonetheless, he praised his rival
Aurobindo, calling it "a totally kosher company," and adding, "As an Indian, I'm
proud of them."
New
AIDS Pill to Treat People in Poor Countries, NYT, 6.7.2006,
http://www.nytimes.com/2006/07/06/world/06aids.html
Mute 19 Years,
He Helps Reveal Brain's
Mysteries
July 4, 2006
The New York Times
By BENEDICT CAREY
HARRIET, Ark., July 2 — Terry Wallis spends
almost all of his waking hours in bed, listening to country-western music in a
cramped, two-room bungalow down a gravel road off State Highway 263.
Mr. Wallis, 42, wears an open, curious expression and speaks in a slurred but
coherent voice. He volleys a visitor's pleased-to-meet-you with, "Glad to be
met," and can speak haltingly of his family's plans to light fireworks at his
brother's house nearby.
For his family, each word is a miracle. For 19 years — until June 11, 2003 — Mr.
Wallis lay mute and virtually unresponsive in a state of minimal consciousness,
the result of a head injury suffered in a traffic accident. Since his abrupt
recovery — his first word was "Mom," uttered at the sight of his mother — he has
continued to improve, speaking more, remembering more.
But Mr. Wallis' return to the world, and the progress he has made, have also
been a kind of miracle for scientists: an unprecedented opportunity to study,
using advanced scanning technology, how the human brain can suddenly recover
from such severe, long-lasting injury.
In a paper being published Monday, researchers are reporting that they have
found strong evidence that Mr. Wallis's brain is healing itself by forming new
neural connections since 2003.
The paper, appearing in The Journal of Clinical Investigation, includes a series
of images of Mr. Wallis's brain, the first such pictures ever taken from a
late-recovering patient.
The new findings raise the hope that doctors will eventually have the ability to
determine which patients with severe brain damage have the best chance of
recovering. They might also help settle disputes in cases like that of Terri
Schiavo, the Florida woman who was removed from life support and died last year
after a bitter national debate over patients' rights. Ms. Schiavo suffered more
profound brain damage than Mr. Wallis and did not show signs of responsive
awareness, according to neurologists who examined her.
"We read about these widely publicized cases of miraculous recovery every few
years, but none of them — not one — has ever been followed up scientifically
until now," said Dr. Nicholas Schiff, a neuroscientist at Weill Cornell Medical
College in Manhattan and the senior author of the new imaging study.
An estimated 100,000 to 200,000 Americans subsist in states of partial or
minimal consciousness, cut off from those around them.
On Saturday, Mr. Wallis said he felt good, but he showed no memory of the study.
After prompting from his mother, he did remember the trip back from the
researchers' laboratory in New York.
"Gasoline," he said, referring to a stop the airplane made to refuel. "We
stopped for gasoline."
His mother, Angilee Wallis, said: "He is starting to learn things now. That
right there is new."
In recent weeks, she said, he has also shown hints of self-awareness, alluding
to his disabled condition for the first time.
Mrs. Wallis, 58, and her husband Jerry, 62, live with and care for their son in
a white clapboard cabin, with a small concrete porch surrounded on all sides by
acres of trees. Their house, between Harriet and Big Flat, is among a scattering
of such hidden homes, sheds and dirt roads a couple of miles from a highway
intersection anchored by two liquor stores. The nearest decent grocery store is
30 minutes away, in Mountain View, Ark.
For the Wallis family, Terry's accident, his long years of mental absence and
his return have been a story of celebrity as well as recovery, of how media
attention can strike like a flash flood and just as quickly dry up, leaving
families to figure out what all the attention meant, if anything — and whether
it was worth it.
He was a lanky 19-year-old in 1984, with a gift for elaborate pranks and engine
work, when he and two friends skidded off a small bridge in a pickup, landing
upside down in a dry riverbed. The family never figured out exactly what
happened. The crash left their son unresponsive, breathing but immobilized,
there but not there, said his father.
Terry Wallis showed no improvement in the first year, and doctors soon
pronounced him to be in a persistent vegetative state, and gave him virtually no
chance of recovery, his parents said.
About 52 percent of people with traumatic wounds to the head, most often from
car accidents, recover some awareness in the first year after the injury,
studies find; very few do so afterward. Only 15 percent of people who suffer
brain damage from oxygen deprivation — like Terri Schiavo, whose heart stopped
temporarily — recover some awareness within the first three months. A 1994
review of more than 700 vegetative patients found that none had done so after
two years.
But at some point after his accident, probably within months, Mr. Wallis, a
mechanic before his injury, entered what is called a minimally conscious state,
Dr. Schiff said. The diagnosis, established formally in 2002, is given to people
who are severely brain damaged but occasionally responsive. In their good
moments, they can track objects with their eyes, respond to commands by
blinking, grunting or making small movements. They may spend the rest of their
lives in this condition, but it is a necessary intermediate step if they are
ever to regain some awareness, neurologists say.
Mr. Wallis spent the second 19 years of his life at a nursing home in Mountain
View, and family members who visited said they saw plenty of hints of awareness
along the way. He seemed to brighten when they walked in his room. Something in
his face would tighten when he was impatient or hungry.
None of which made the day he said "Mom" any less thrilling. Ms. Wallis, her
voice unsteady, quickly put out the word to the extended family.
Later, the patient had another visitor, a striking blonde woman: his 19-year-old
daughter, Amber, who had been 6 weeks old at the time of his accident. "I was so
nervous driving over there," she said. "I was looking in the rearview mirror to
check my hair, I swear, I was so worried he wouldn't recognize me."
When finally he did, she said, the first sentence he uttered was, " 'You're
beautiful,' and he told me he loved me."
He was suddenly speaking; it was a transformation. He was still disabled, barely
able to move or speak, but he was recognizable as Terry.
The months that followed brought a swarm of other emotions. Mr. Wallis, now
considered clinically recovered but still in need of around-the-clock attention,
was moved into his parents' home, shifting much of the financial burden of his
care from Medicaid to them.
And the world came knocking. A camera crew from Japan arrived and spent two
weeks doing daily interviews and filming. Another crew visited from England.
There were talk show appearances, agents, documentary makers, forcing Mrs.
Wallis to take time away from her job at a local shirt factory to help her
husband, a mechanic and farmer, play host.
But the attention soon dissipated, and a fund his parents established for their
son's care — the Terry Wallis Special Needs Trust — attracted few substantial
contributions, they said.
Their son still needed to be fed, washed, exercised and turned in his bed every
two hours, night and day. His daughter took two regular shifts a day to tend to
him, and another aide began working with the family.
But in some ways it was like living with a child who never grows up or leaves
home: there, out back in the trees, was his old gray Ford van, untouched since
1984; out front was an aluminum boat his father had bought for him, overturned,
unused.
In 2004, Dr. Schiff contacted the family, asking if they would allow their son
to be studied. He helped arrange to have the Wallises flown to New York in April
of that year, and again 18 months later, for brain scanning. A research team
from New York, New Jersey and New Zealand spent more than a year analyzing the
results, comparing them to images from healthy brains and from another minimally
conscious patient who had not recovered.
Using a novel technique, they saw evidence of new growth in the midline
cerebellum, an area involved in motor control, as Mr. Wallis gained strength and
range in his limbs. Another area of new growth, located along the back of the
brain, is believed by some experts to be a central switching center for
conscious awareness.
The daily exercises, the interactions with his parents, his regular dose of
antidepressant medication: any or all of these might have spurred brain cells to
grow more connections, the researchers said.
"The big missed opportunity is that we didn't know this guy would spontaneously
emerge, and we didn't get to monitor him before then" to find out what preceded
it, Dr. Schiff said.
To answer that kind of question in a systematic way, researchers will need to
follow more minimally conscious patients for longer periods, experts say. But
there is no national system to track such patients, they say, no central
database like that which exists for other diseases.
"We don't see these people. They exist outside of our gaze. We don't even know
where they live," said Dr. Joseph Fins, chief of the medical ethics division of
New York Presbyterian Hospital-Weill Cornell Medical Center.
Mr. Wallis, it was clear over the weekend, continues to live for the day. He has
a granddaughter now, Amber's child, Victoria, and the 2-year-old does not seem
bothered by the pale man with the dark mustache and the inward-turned arms. He
does not feel any physical pain, he told his parents, and he has no real sense
of time. He also said recently that he was "proud" to be alive.
"It is good to know all that," said his father, sitting on the porch on Saturday
evening.
"It's good to hear him say that, because if he didn't say so, you'd just have no
way to know."
Mute
19 Years, He Helps Reveal Brain's Mysteries, NYT, 4.7.2006,
http://www.nytimes.com/2006/07/04/health/psychology/04coma.html
A Warning on Hazards of Secondhand Smoke
June 28, 2006
The New York Times
By JOHN O'NEIL
The evidence is now "indisputable" that
secondhand smoke is an "alarming" public health hazard, responsible for tens of
thousands of premature deaths among nonsmokers each year, Surgeon General
Richard H. Carmona said yesterday.
Dr. Carmona warned that measures like no-smoking sections did not provide
adequate protection, adding, "Smoke-free environments are the only approach that
protects nonsmokers from the dangers of secondhand smoke."
He did not call for a federal ban on smoking in workplaces, bars or restaurants,
a step that has been taken by a growing number of cities and states over the
objections of business owners and of groups skeptical about the dangers of
secondhand smoke. He said he saw his role as providing the public and Congress
with definitive information on the subject.
"I am here to say the debate is over: the science is clear," Dr. Carmona said at
a televised news conference, where he released a report updating the original
surgeon general's study of secondhand smoke in 1986. Since then, hundreds of
studies have indicated that the harm caused by secondhand smoke is far greater
than earlier believed, he said. The report includes these findings:
¶There is no safe level of secondhand smoke, and even brief exposure can cause
harm, especially for people suffering from heart or respiratory diseases.
¶For nonsmoking adults, exposure raises the risk of heart disease by 25 percent
to 30 percent and of cancer by 20 percent to 30 percent. It accounted for 46,000
premature deaths from heart disease and 3,000 premature deaths from cancer last
year.
¶Secondhand smoke is a cause of sudden infant death syndrome, or SIDS,
accounting for 430 deaths last year. The risk is elevated for children whose
mothers were exposed during pregnancy and for children exposed in their homes
after birth.
¶The impact on the health and development of children is more severe than
previously thought. "Children are especially vulnerable to the poisons in
secondhand smoke," Dr. Carmona said.
¶Efforts to minimize the effect of secondhand smoke by separating smokers and
nonsmokers are ineffective, as are ventilation systems in a shared space.
¶While exposure has declined, as many as 60 percent of nonsmokers show
biological evidence of encountering secondhand smoke, and 22 percent of children
are exposed to secondhand smoke in their homes.
Studies conducted by the Centers for Disease Control show that great progress
has been made in reducing exposure, Dr. Carmona said. The amount of cotinine —
the form nicotine takes after being metabolized — in blood samples fell by 75
percent among adults, according to specimens taken from 1999 to 2002 that were
compared with samples taken a decade earlier.
But Dr. Carmona said more needed to be done, particularly to protect children.
He urged parents who smoke not only to quit, but also to move their smoking
outside while trying to quit. "Make the home a smoke-free environment," he said.
Tobacco companies say the risks of secondhand smoke are unproved and overstated.
In a statement on its Web site, R. J. Reynolds says, "It seems unlikely that
secondhand smoke presents any significant harm to otherwise healthy nonsmoking
adults; and, given the extensive smoking bans and restrictions that have already
been enacted, nonsmokers can easily avoid exposure to secondhand smoke."
A spokesman for the company, David Howard, said yesterday, "Bottom line, we
believe adults should be able to patronize establishments that permit smoking if
they choose to do so," according to The Associated Press.
Dr. Cheryl G. Healton, the president and chief executive of the American Legacy
Foundation, a nonprofit group created to use settlement money from tobacco
companies to educate young people about the dangers of tobacco, called the
surgeon general's report "groundbreaking" even though much of its information
had already been published in journal articles. Bringing it all together creates
a persuasive case for smoking bans, Dr. Healton said.
The report is online at surgeongeneral.gov/library/secondhandsmoke/.
A Warning on Hazards of Secondhand Smoke, NYT, 28.6.2006,
http://www.nytimes.com/2006/06/28/health/28smoke.html
Related >
http://surgeongeneral.gov/library/secondhandsmoke/
Charities Tied to Doctors
Get Drug Industry
Gifts
June 28, 2006
The New York Times
By REED ABELSON
As she presented research results indicating
that a new medical device was "an important breakthrough," the doctor's
enthusiasm was clear. Less evident were some of the financial links between the
researchers and the device's maker.
Dr. Maria Rosa Costanzo, making her presentation at a March conference of
cardiologists, said the study found that a $14,000 blood filtering device was
better than intravenous diuretic drugs at removing excess fluid from patients
with heart failure.
Although outside researchers raised questions about the study's conclusions, the
doctor betrayed little doubt. "We believe these results challenge current
medical practice and recommendations," said Dr. Costanzo, who predicted many
patients might benefit.
Dr. Costanzo did disclose to the audience that she was a paid consultant with
stock in the device's maker, a Minnesota company called CHF Solutions. But she
omitted another potentially important detail: CHF Solutions was also one of the
largest donors to the nonprofit research foundation that had overseen the study.
The company contributed about $180,000 in 2004, according to the foundation's
federal filings.
Nor did she note that the nonprofit entity, the Midwest Heart Foundation, was in
turn an arm of the thriving for-profit medical group outside of Chicago where
Dr. Costanzo and more than 50 of her fellow doctors treat heart patients — in
many cases using products and drugs made by CHF Solutions and other big donors
to their charity. Although the CHF Solutions device has generally been slow to
catch on, physicians at Dr. Costanzo's medical group have treated many patients
with the company's filtration system.
The Midwest Heart Foundation, and the way it has become quietly interwoven into
its doctors' professional lives, is far from unique. Around the country, doctors
in private practice have set up tax-exempt charities into which drug companies
and medical device makers are, with little fanfare, pouring donations — money
that adds up to millions of dollars a year. And some medical experts see that as
a big problem.
The charities are typically set up to engage in medical research or education,
and the doctors involved defend those efforts as legitimate charitable
activities that benefit the public. But because they operate mainly under the
radar, the tax-exempt organizations represent what some other doctors, as well
as regulators and industry consultants, say is a growing conduit for industry
money. The payments, they say, can bias the treatment decisions of physicians,
may lead to suspect research findings and at times may even risk running afoul
of anti-kickback laws.
Federal officials are starting to take notice of such tax-exempt charities,
which critics say are becoming increasingly popular as other forms of industry
support to physicians — like lucrative consulting agreements that involve little
actual work — have come under scrutiny from regulators and others worried about
the potential conflicts.
The potential for abuse by these charities is clear, critics say. "It obviously
sets a fertile ground for conflict of interest and misuse of funds," said Dr.
Robert M. Califf, vice chancellor for clinical research at Duke University
Medical Center.
The charities at issue are not philanthropies like the Bill and Melinda Gates
Foundation that dispense grants for medical research but remain independent of
any one group of doctors or medical practice. Instead, the charities drawing
scrutiny are set up by doctors in private practice and are closely linked to
those doctors' for-profit medical groups.
The Midwest Heart Foundation, which has received millions of dollars from
medical industry donors, including the drug makers Amgen and AstraZeneca, and
the Cordis and Scios units of Johnson & Johnson, says it stands behind its
charitable work, which currently involves about 30 studies and dozens of
doctor-education lectures each year.
Dr. Mark Goodwin, a managing partner for the Midwest Heart for-profit practice,
said the foundation was created to help prevent potential conflicts by keeping
the industry money separate from the doctors' private practice. Companies
contribute to the foundation, he said, because they can rely on its research and
the doctors involved can enroll large numbers of patients in studies. "We are
able to deliver excellent research to our community in a timely fashion," Dr.
Goodwin said, "and we are proud of it."
But some of its research has drawn criticism from federal regulators. Earlier
this year, moreover, the foundation received a Justice Department subpoena as
part of an investigation into the marketing activities of one of its big
contributors, Scios.
Experts aware of the various doctor-run charities say that even if much of the
donated money is spent on legitimate medical research or education, the funds
can also go toward studies that while lending prestige to the doctors and luster
to the companies, may do little to advance scientific understanding. The
tax-exempt money also sometimes flows to the for-profit medical groups
affiliated with the charities, sometimes covering business expenses or even
paying parts of the salaries of doctors.
Too often, the critics contend, the industry donations amount to a form of
"relationship funding" — to use one skeptical doctor's term — in which companies
hope to sell more drugs and devices by currying favor with the doctors. That
skeptic, Dr. John Cherf, is a knee surgeon at the Neurologic and Orthopedic
Institute of Chicago who also consults for a market research firm specializing
in health care topics. He says the donor arrangements are fraught with potential
conflicts of interest and are likely to come under greater scrutiny as the costs
of devices and drugs rise.
"There's undoubtedly corruption in the system," Dr. Cherf said. "We need healthy
relationships between physicians and industry. Both parties have been too
aggressive."
Number of Charities Is Unknown
No one knows precisely how many of these doctor-run charities exist. Although
each one files with the federal government as a tax-exempt entity, they are hard
to discern among other health-related charities. And because in many cases each
has no more than a few hundred thousand dollars in annual revenue, they tend to
escape the attention of the federal and state regulators who oversee charities.
"The reality of it is that these are small organizations that are off the radar
screen," said Douglas M. Mancino, a lawyer at McDermott Will & Emery in Los
Angeles who specializes in health care law and nonprofit groups.
As long as the activities being financed benefit the public rather than the
doctors or companies involved, they are legitimate charities, according to
lawyers who specialize in nonprofits.
But concerns can arise when a corporate donation appears to be helping pay the
salary of an additional doctor at a for-profit medical practice — through a
fellowship, for example — that brings in additional revenue to the practice.
Another problem area, they say, would be when donations go toward expenditures
that would normally be part of the practice's business cost.
Lawyers say that determining whether a charity's activities are legitimate
tax-exempt activities would typically require a close look at the facts in each
case.
"If they're really underwriting normal business expenses to the group, then I
think you have a problem," Mr. Mancino said.
As a group, these relatively obscure charities are attracting sizable amounts of
corporate money. And many of their activities focus on the companies that have
made the donations or the doctors' medical groups.
Consider the Arizona Orthopedic Education Foundation, which was created by a
surgeon in Phoenix and which in 2003 received a $200,000 donation from a unit of
the orthopedic device company Stryker. Most of the charity's efforts are devoted
to public education, according to the founder, Dr. Anthony K. Hedley. But its
activities also include teaching other doctors how to use Stryker products.
Stryker said this training was "critical" for surgeons.
Dr. Hedley says the fact that he mainly uses Stryker devices with his own
patients may account for Stryker's contributions. "That was probably why I was
able to leverage support," Dr. Hedley said.
Another charity is the Blue Ridge Bone and Joint Research Foundation, run by Dr.
Joseph T. Moskal, an orthopedic surgeon in Roanoke, Va. It received a $75,000
contribution from the DePuy Orthopaedics unit of Johnson & Johnson in the year
ended July 31, 2004, according to federal filings. The Blue Ridge foundation
appears to have paid $30,000 of that money to the for-profit Roanoke Orthopaedic
Center, where Dr. Moskal practices, to defray the costs of a fellowship program
there.
Dr. Moskal did not return repeated phone calls seeking comment. DePuy, in a
brief response to questions, said in part, "Fellowships are vital to advance the
education and training of orthopaedic surgeons."
Corporate donors are also major contributors to the Vascular Specialists
Education Foundation, which is led by a vascular surgeon in Norfolk, Va., Dr.
Marc H. Glickman. The foundation spent $30,000 in 2003 to pay for the further
medical education of doctors in his for-profit practice.
Although the public filings offer few details about the charity's activities,
Dr. Glickman said such expenditures are part of the foundation's mandate, which
includes offering fellowships to doctors being trained and paying for continuing
medical education for those doctors. One of Vascular Specialists' two big
donors, the device maker Guidant, now part of Boston Scientific, said it
contributed $25,000 in 2003 and $40,000 the next year, through its own
foundation. The company says the money was given with the understanding that it
would go to finance the group's fellowship program.
The other big donor, the device maker Medtronic, says it gave Dr. Glickman's
charity $80,000 last year to help pay for the group's fellowship program. "Dr.
Glickman and his colleagues have trained hundreds of physicians and fellows on
life-saving procedures associated with vascular disease — a notable
accomplishment," Medtronic said in a written statement.
Donors have been so generous to Dr. Glickman's foundation that he says it is
currently sitting on $100,000 he has not yet decided how to spend. "I'm very
cautious with what I do," he said.
Whatever the issues of tax-exempt status among the various charities, federal
regulators say the groups could find themselves in trouble in another way — in
violation of federal anti-kickback laws — if donations appear to be little more
than a way for companies to funnel money to doctors.
If the contributions amount to payments or gifts to doctors who then use or
recommend a certain drug or device, companies could be breaking the law, said
Vicki Robinson, a top lawyer in the Office of Inspector General at the federal
Health and Human Services Department.
"From a legal perspective, it's really no different," Ms. Robinson said.
Patrick L. Meehan, the United States attorney in Philadelphia, whose office has
a long history of prosecuting health care fraud, said the doctors' charities
could warrant scrutiny. "What we would be concerned about are end runs around
the system," Mr. Meehan said. "We want to be sure there is independent and fully
informed medical judgment at the heart of the physician-patient relationship."
For their part, Midwest Heart officials defend the activities of their
foundation. Contributions to the charity, which was created in 1988, have more
than doubled in the last few years — to $1.7 million in 2004, the most recent
period for which federal filings are available.
In a written statement, the foundation said it had "strict internal controls and
systems in place to ensure the independence and integrity of all research and
education activities."
Questions About Research
Outside researchers have questioned some of the foundation's work. Some doctors
say the study of the CHF Solutions filtration device that Dr. Costanzo presented
in March may have been flawed, for example, because heart failure patients who
were given conventional diuretic drugs may not have received enough medicine to
provide meaningful comparisons.
One heart doctor critical of those findings was Dr. JoAnn Lindenfeld, who was
quoted in a cardiology publication, Heartwire, in March as saying, "I wouldn't
view these data as persuasive enough to use it full-scale in a million patients
a year with acute decompensated heart failure." Dr. Lindenfeld did not dispute
the accuracy of that quote but declined to comment further.
Through the Midwest Heart Foundation, Dr. Costanzo declined to comment. Both CHF
Solutions and the foundation say she no longer has stock or stock options in the
company.
CHF Solutions said that most of its contributions to the Midwest Heart
Foundation covered the cost of conducting the research project that Dr. Costanzo
led and the company helped design.
John L. Erb, CHF's chief executive, said "we were very careful" in designing the
research, but he conceded that it was "not the perfect study where we could
answer all the questions."
Dr. Goodwin, at the foundation, said the research was only a starting point. "We
fully agree that further investigation is needed to validate the findings and
carry them forward to a larger number of patients," he said.
Some of Midwest Heart's research has also fallen short of federal rules
governing clinical studies. In August 2004, the Food and Drug Administration
sent the foundation a warning letter about a study of a new carotid stent — a
device designed to open up a major artery in the head and neck.
The F.D.A. said Midwest Heart had failed to get necessary approval before
beginning its research, which involved different types of stents and 168 patient
procedures. The regulators also found that some patients were not properly
informed and that the foundation was too slow in reporting serious
complications. The results of the study were never published, although the
foundation says they were submitted to the F.D.A.
The shortcomings were simply "record keeping" issues, said Wendy Landow, the
chief executive of the Midwest Heart Foundation, who said her organization had
in fact received the necessary approval to do the study but had poorly
documented it. The issue has been resolved, she said, adding that the foundation
had adopted tighter procedures to avoid future lapses.
A separate controversy surrounds the heart failure drug Natrecor made by Scios,
which gave the Midwest Heart Foundation a total of more than $300,000 for the
years 2003 and 2004, according to federal filings. The Justice Department, which
is investigating whether Scios improperly marketed Natrecor, has issued a
subpoena to the foundation.
Scios said that most of its Midwest Heart contributions went toward educational
programs that Scios had no influence over. It said it could not comment on the
Justice Department investigation. Midwest Heart said it was cooperating with
federal officials and had been told it was not a target of the investigation.
Natrecor was approved by the F.D.A. in 2001 for use in hospitals for patients
only in an extreme, or decompensated, stage of heart failure. But it also became
heavily used by doctors who administered it intravenously in outpatient clinics
for periodic patient "tune-ups," as they were sometimes known. Natrecor's
enthusiasts included some Midwest Heart doctors, who participated in studies of
the drug and also used it in outpatient settings.
While doctors can use federally approved drugs for any purpose they see fit, a
pharmaceutical company is prohibited from actively encouraging such off-label
uses.
A Debate Over Drug's Merits
In mid-2005, after researchers elsewhere published an article in a scholarly
medical journal raising concerns that Natrecor could seriously impair kidney
function, one of Midwest Heart's cardiologists, Dr. Mitchell T. Saltzberg,
continued to staunchly defend the drug. Dr. Saltzberg, who has also been a paid
Scios consultant, wrote to Medicare officials in July 2005 to argue that the
drug was being "unfairly targeted."
Dr. Saltzberg's letter cited a study of Natrecor's outpatient use — a study for
which the foundation had provided some work — saying that this research and "the
body of anecdotal experience" indicated the drug posed no kidney risks.
His comments to Medicare, though, came a few days after Scios itself sent a
safety alert to doctors warning against the outpatient use of Natrecor. The
Scios alert, issued in consultation with the F.D.A., relied on the findings of
an expert panel that the company had asked to look into issues involving the
drug's safety.
The Scios alert referred to the very study Dr. Saltzberg had cited and found it
lacking. That study "was not powered to adequately assess the effectiveness or
safety of serial infusions of Natrecor," the alert said. "The size of the study,
its design and its findings provide an inadequate basis to recommend the use of
intermittent, serial or scheduled repetitive infusions of Natrecor." Through the
foundation, Dr. Saltzberg declined to comment. Foundation officials, though,
said they agreed with the Scios panel's findings.
Outpatient use of Natrecor around the country has fallen precipitously. Scios
has said it plans to conduct further research into the drug's safety.
The Midwest Heart Foundation said that only one of its patients, who is part of
a study, is still being given the drug as an outpatient. But while the
foundation says it believes more research is needed, Dr. Goodwin also said that
he believes that many doctors had positive results with the drug and that he had
seen it keep patients out of the hospital.
"It worked great," he said.
Charities Tied to Doctors Get Drug Industry Gifts, NYT, 28.6.2006,
http://www.nytimes.com/2006/06/28/business/28foundation.html
Buffett's Billions Will Aid Fight Against
Disease
June 27, 2006
The New York Times
By DONALD G. McNEIL Jr. and RICK LYMAN
Warren E. Buffett's $31 billion gift to the
Bill & Melinda Gates Foundation will help the foundation pursue its longstanding
goal of curing the globe's most fatal diseases, Mr. Gates said yesterday, along
with improving American education.
The foundation hopes to use the enormous gift, among other things, to find a
vaccine for AIDS, Mrs. Gates said. And Mr. Gates went further, saying that while
he might be "overly optimistic," he believed there was a real shot at finding
cures for the 20 leading fatal diseases, as well as ensuring that every American
has a chance at a decent education.
"Can that happen in our lifetime?" Mr. Gates said, sitting next to Mr. Buffett
at the New York Public Library, where the gift was formally announced after news
of it broke on Sunday. "I'll be optimistic and say, Absolutely."
But Mr. Gates acknowledged that spending the money effectively would be
difficult. The scientific tasks the foundation has set for itself in fields like
malaria and tuberculosis take time as well as money, because they require years
of laboratory work followed by years of clinical trials, sometimes ending
fruitlessly. Improving American education — once better ideas have been found —
can take just as long.
"It's incredibly difficult to give this much money away well," said Jean
Strouse, a biographer who has compiled an oral history project on the Gates
Foundation. "And giving it away to people who can use it well, especially in
places where poverty is so overwhelming, where there's not much real
infrastructure."
Both Mr. Buffett, who will join the foundation's leadership, and the Gateses
acknowledged as much.
"In the last few months we have begun to really talk about and try to come up
with a plan for that," Mrs. Gates said.
They must, for instance, improve their dialogue with the governments of poor
nations to make sure that vaccines get down to the people who need them.
Mr. Buffett, for his part, said he saw no need to tinker with the foundation's
essential goal: improving the lot of poor people elsewhere in the world without
regard to their color, religion or other differences.
Describing his own way of choosing companies to invest in, Mr. Buffett, one of
history's most successful investors, said, "I've learned to adapt to other
managers" and then jokingly compared the process to picking a spouse. "It's not
a good idea to marry one expecting them to change," he said.
Mrs. Gates was a Microsoft executive when she married Mr. Gates when he was 38
and she was 29. Upon hearing Mr. Buffett's remark, Mr. Gates leaned back on his
stool with a big sheepish grin as his wife glanced knowingly at him.
Then Mr. Buffett said, "I'm happy with the ones I'm marrying here."
Later in the exchange, which was in front of 200 philanthropy executives,
scientists, students and a few reporters, Mr. Gates got in his own reflection on
the partnership. "It's scary," he said. "If I make a mistake with my own money,
it isn't as big as making a mistake with Warren's money."
To which Mr. Buffett replied: "I won't grade you more often than daily."
Mr. Buffett is giving away about 85 percent of his fortune, most of it to the
Gates foundation. The gift, representing the current value of 10 million Class B
shares of Berkshire Hathaway, the insurance conglomerate he formed nearly 50
years ago, will nearly double the wealth of the Gates Foundation, which was
already the world's biggest, at almost $30 billion. The stock will be
transferred to the foundation in increments over many years; the first transfer
will be half a million shares this year, worth about $1.5 billion.
Although the money will not change the foundation's larger goals, Mrs. Gates
mentioned yesterday that it had been moving quietly for the last 18 months into
microlending, which is the granting of small loans to poor people so they can
start small businesses. A microloan of less than $50 might finance, for example,
the purchase of a loom or a set of bicycle repair tools.
Though he is also leaving billions to separate foundations for his children, Mr.
Buffett said he felt he was "not cut out" to be a philanthropist like the
Gateses and preferred to remain at the helm of his company.
"They'll spend more time and energy on it," he said. "I'm having so much fun
doing what I do, and I think they'll be more able to accept any mistakes they
made than I would if I made them."
Bill Gates was a quicker study on new topics, like medicine, that he would have
to master, Mr. Buffett said, and added: "I wouldn't want to listen to as many
people with as many different opinions as they do."
Rather than spend every cent on fruitlessly trying to rebuild broken health care
systems, the Gates Foundation follows a pattern of spending generously to chase
solutions like a malaria vaccine. It also buys supplies, like vaccines or
mosquito nets, but then tries to get rich countries to match its donations and
poor countries to get organized well enough to distribute the goods.
Similarly, in education, it creates model schools that public school systems can
use as examples, rather than spending endlessly to pay the expenses of every
impoverished American school district.
Her "fondest dream," Mrs. Gates said, is an AIDS vaccine, something scientists
have been pursuing since the 1980's and which she admitted could take an
additional 20 years. A stopgap measure, she said, could be a microbicide: an
undetectable protective gel that women could insert before sex.
Mr. Gates said he wanted to use improved global health as a base upon which to
build what he called "the virtuous cycle" of longer lifetimes, jobs, markets,
infrastructure, tax bases and all the other steps that lift poor countries out
of poverty.
Dr. Richard Klausner, a former director of the National Cancer Institute and the
Gates Foundation's former head of global health, said that besides microlending
he also would not be surprised if the foundation followed the Rockefeller
Foundation's example in seeking higher-yield, drought-resistant seeds for poor
farmers.
Dr. Harold E. Varmus, president of the Memorial-Sloan Kettering Cancer Center,
said the foundation could fight some of the major preventable causes of death in
poor countries: cigarettes, alcohol abuse and automobile injuries.
Dr. Varmus was the chief scientific adviser for the Grand Challenges in Global
Health, a sort of contest in which Mr. Gates gave out $437 million to teams
pursuing exotic goals like vaccines that can be inhaled or chemicals that can
knock out mosquitoes' sense of smell. He said his advisory committee
particularly wished it could make grants for water purification and for chronic
diseases like diabetes and cancer that have loomed larger in the poor world as
people live longer.
Asked if a richer Gates Foundation could divert scientists from other fields,
Dr. Varmus said he was "more concerned with using the scientific horsepower
we've already developed."
Noting that the National Institutes of Health give out $28 billion a year — ten
times as much as even the enriched Gates Foundation will — he said its
inflation-adjusted budget has been shrinking.
Some aid recipients also worry that the Gates-Buffett fortune will let other
donors, including the American government, feel that they can back away from
public health. That would be disastrous for the world's poor, they said, since
the foundation is only one stream in a vast river. If anyone does back away, Dr.
Klausner said "it's because they were looking for an excuse, not because there's
no need."
Diana Aviv, president of Independent Sector, a nonpartisan coalition that
represents charities and foundations, said she expected the Buffett money to
give the Gates Foundation more power.
"They haven't served multiple programs," Ms. Aviv said. "They've been much more
generous in a few. This gives them leveraging opportunities."
Mr. Buffett said yesterday that he was a student of the same philanthropists
that Mr. Gates modeled himself on: the oilman John D. Rockefeller; the steel
magnate Andrew Carnegie; Irene Diamond, the widow of the real estate developer
Aaron Diamond; and Joan Kroc, the widow of Ray Kroc, who founded McDonald's.
Mr. Buffett is also famous for loving efficiency. He runs a company with 200,000
employees from an Omaha headquarters with fewer than 20 employees. The Gates
Foundation, in Seattle, has about 300.
Mr. Buffett was scathing yesterday in describing his feelings about estate
taxes, which the Bush administration is trying to kill. The ability of rich men
to pass on "dynastic wealth" to their grandchildren is offensive to the American
tradition of meritocracy, he said.
He gets particularly upset at his country club, he said, hearing members
complain about welfare mothers getting food stamps "while they are trying to
leave their children a more-than-lifetime-supply of food stamps and are
substituting a trust officer for a welfare officer."
To widespread applause, he smiled and asked: "Is there anyone I forgot to
insult?"
Buffett's Billions Will Aid Fight Against Disease, NYT, 27.6.2006,
http://www.nytimes.com/2006/06/27/us/27gates.html
The DNA Age
That Wild Streak?
Maybe It Runs in the
Family
June 15, 2006
The New York Times
By AMY HARMON
Jason Dallas used to think of his daredevil
streak — a love of backcountry skiing, mountain bikes and fast vehicles — as "a
personality thing."
Then he heard that scientists at the Fred Hutchinson Cancer Research Center in
Seattle had linked risk-taking behavior in mice to a gene. Those without it
pranced unprotected along a steel beam instead of huddling in safety like the
other mice.
Now Mr. Dallas, a chef in Seattle, is convinced he has a genetic predisposition
for risk-taking, a conclusion the researchers say is not unwarranted, since they
believe similar variations in human genes can explain why people perceive danger
differently.
"It's in your blood," Mr. Dallas said. "You hear people say that kind of thing,
but now you know it really is."
A growing understanding of human genetics is prompting fresh consideration of
how much control people have over who they are and how they act. The recent
discoveries include genes that seem to influence whether an individual is fat,
has a gift for dance or will be addicted to cigarettes. Pronouncements about the
power of genes seem to be in the news almost daily, and are changing the way
some Americans feel about themselves, their flaws and their talents, as well as
the decisions they make.
For some people, the idea that they may not be entirely at fault for some of
their less desirable qualities is liberating, conferring a scientifically backed
reprieve from guilt and self-doubt. Others feel doomed by their own DNA, which
seems less changeable than the more traditional culprits for personal failings,
like a lack of discipline or bad childhoods. And many find it simply depressing
to think that their accomplishments might not be the result of their own
efforts.
Parents, too, are rethinking their contributions. Perhaps they have not scarred
their wayward children so much as given them bad genes. Maybe it was not their
superior parenting skills that produced that Nobel laureate.
Whether a new emphasis on genes will breed tolerance or bigotry for inborn
differences remains an open question. If a trait like being overweight comes to
be seen as largely the result of genetic influence rather than lack of
discipline, the social stigma connected to it could dissipate, for instance. Or
fat people could start being viewed as genetically inferior.
Because tests for the genes that influence personality and behavioral traits are
not yet commercially available, there is no way for most people to know which
ones they have. And even if they could, the newly uncovered genes are thought
merely to influence, not determine, their personalities. Biologists are also
quick to emphasize the role environment plays in activating genetic dispositions
that might otherwise never be expressed, or mitigating those that are.
But that has not stopped people from acting on their assumptions.
Mr. Dallas's wife, Mari, for instance, convinced that her husband is in some
sense hostage to his daredevil genes, has insisted he draw the line at certain
activities.
"If he had his choice, he would be getting a motorcycle," said Ms. Dallas, a
pediatric oncologist. "I don't think that's such a good idea."
The public embrace of genetics may be driven as much by wishful thinking as
scientific truth. In an age of uncertainty, biology can appear to provide a
concrete answer for behavior that is difficult to explain. And the faith that
genetics can illuminate the metaphysical aspects of being human is for some a
logical extension of the growing hope that it can cure disease.
"More and more stories about who we are and how we live are becoming molecular,"
said Paul Rabinow, an anthropologist at the University of California, Berkeley,
who studies the interrelation of science and culture. "The older liberal
worldview that it's all a question of willpower is still very present in
America, but genetics has become a strong countercurrent."
That may be partly because the science has become more credible. Armed with the
human genome sequence, along with a catalog of genetic variation in the human
population, and tools that can inexpensively gauge any individual's genetic
makeup, scientists can now pinpoint the genes associated with inherited traits.
Developed to dissect the genetic basis for complex ailments like heart disease
and cancer, the methods are now being applied to less pressing areas like the
way genes may influence sexual desire or attention deficit disorder. While
scientists have yet to demonstrate any genetic cause that directly affects such
behavior, they have found plausible associations. And for many people, that is
all that matters.
"The scientific facts have changed," said Steven Pinker, a psychologist at
Harvard who documented cultural resistance to the influence of genetics on
behavior in his 2002 book "The Blank Slate."
"We now have real evidence that some of the variation in personality is
inherited," Dr. Pinker said, "and I think it may be affecting people's everyday
choices."
Some people persist in believing in the power of the human spirit, but a growing
number prefer to submit it to a DNA test. In the wake of the recent discovery
that millions of people who carry a specific genetic variation are more likely
to gain weight, Mike DeWolfe, a computer programmer who considers himself
overweight, cannot help wondering if he is one of them.
"I really would like to have a test, because it would help reduce my guilt over
it," said Mr. DeWolfe, 38, of Victoria, British Columbia, noting he would also
welcome a genetic treatment as an alternative to his constant dieting. "That
would make a big difference."
There is nothing new about the idea that temperament and behavior are shaped by
genetic endowment. Families have long clucked over a trademark stubborn streak
showing up in a new generation, or crowed about inherited creative abilities.
But as science begins to corroborate intuition, the public is reassessing where
credit and responsibility lie for character traits that may be in part
genetically preordained.
"To summarize, want to live until a ripe old age? Have parents that live long,"
Joe Pickrell, a 23-year-old graduate genetics student wrote in a recent blog
entry. "Think you're a friendly, peaceful guy 'cause your mom raised you right?
Think again. Able to try drugs just a couple times and never get hooked because
of your strong will? Nope." (Mr. Pickrell, of Chicago, punctuated each clause
with a link to a recent scientific journal article describing the genetic
component of life expectancy, aggression and susceptibility to drug addiction.)
Jacki Thorpe wondered for years why her older sister could quit smoking so
easily, while her own numerous attempts have failed. After all, their upbringing
had been virtually identical, and they had started smoking together when they
were 12 and 14. Then she heard about a genetic variation that predisposes some
people to nicotine addiction.
"I have it," guessed Ms. Thorpe, 42, an administrative assistant in Whidbey
Island, Wash. "My sister doesn't." Determined to fight her presumed genetic
destiny, Ms. Thorpe has sworn to try quitting one more time this summer.
A Stanford University student in a focus group on smoking and genetics was more
accepting: "Let's say I'm still addicted to cigarettes 10 years from now," the
student said in a telephone interview, asking that his name not be used because
he has concealed his smoking habit from his family. "It might feel like it's not
a total personal failure, just that certain things made it harder for me than
other people. It kind of takes the weight off."
Friends and family members who worry about behavior that seems unhealthy or
self-destructive sometimes suspect that blaming genes is an easy out. When
Representative Patrick J. Kennedy, Democrat of Rhode Island, cited his family's
history of addiction in admitting to a prescription drug addiction after he
crashed his car near the Capitol last month, for instance, some scoffed.
"Kennedy blames crash on 'car accident gene,' " read the headline on
Antimatternews.com, a satirical blog, an allusion to the 1969 crash in which his
father, Senator Edward M. Kennedy, was driving and a passenger was killed. Some
bioethicists warn that the embrace of genetics as an explanation for troubling
behavior threatens to let society off the hook, too. Taxing cigarettes, banning
smoking in bars and not glamorizing it in movies is far more likely to lower
smoking rates than drugs tailored to certain genotypes, these critics say.
Still, at Hazelden, an addiction-treatment center in Minnesota, teaching about
genetics has become standard. Learning that roughly half the risk of alcohol
addiction is associated with genes can remove a burden of guilt that otherwise
serves as an obstacle to recovery, said Dr. Marvin D. Seppala, the center's
chief medical officer.
"They've driven drunk, and they have children, and they're saying, 'I can't
believe I did this,' " Dr. Seppala said. "To learn they have a disease with a
genetic component like other diseases really helps them understand these crazy
sort of behaviors."
As genetics comes to rival childhood experience as the favored lens through
which to interpret behavior seen as deviant, parents who blamed themselves for
their children's disorders are also finding some relief. Recent research has
found that conditions like anorexia or autism, once thought to be largely
psychological, are at least partly genetic.
"You would wonder, 'What's wrong, what aren't we providing?' " said Kathy
Ramsay, 55, a legal secretary in Sacramento who has had three daughters who
suffered from anorexia. The new DNA paradigm, however, can come with a new guilt
trip.
"I passed it on to them," added Ms. Ramsay, whose daughter Heather volunteered
for a genetic study of anorexia at the University of North Carolina after
reading about the research in her local newspaper this year. "It was in me."
Some adults are more forgiving of parents' sins they now consider DNA-enabled.
Others get angry, however irrationally, for being saddled with inferior genes.
Tim McGrath, 45, said learning about the genetics of alcoholism had made him
more determined not to follow the path of his father. Still, he is haunted that
he has seen his own fate.
"It's like this demon out there, lurking," said Mr. McGrath, a teacher in
Chicago. "And without the proper vigilance, or whatever, it could strike."
By suggesting a genetic basis for behavior previously believed by some to be the
result of character flaws, scientists and others say the discoveries could make
for more understanding of human differences. Some overweight people, for
instance, hope it will reduce the stigma associated with being fat.
"Maybe it will help the rest of the world realize it's not lack of willpower,
it's not stubbornness, it's not laziness," said Jane Perrotta, 52, a medical
writer and contributor to the weight-loss blog The Skinny Daily Post.
"It's the hand you're dealt," Ms. Perrotta said.
Others fear that when certain behaviors once ascribed to personal choice are
seen as genetic, the next step will be not tolerance for difference, but support
for intervention. On a "fat-acceptance" e-mail list, several members suggested
recent research will lead only to new ways for them to lose weight through
genetic alteration, rather than be accepted as they are. And when scientists
caused fruit flies to pursue flies of the same sex by altering a gene last year,
some gay-rights advocates worried it would lend credence to the notion that
homosexuality could be "cured."
People could also find their genes being held against them. Already, some
scientists suspect a specific gene plays a role in violent behavior, for
instance, and a discussion has already begun over how people bearing such genes
should be treated.
"If we find a murder mutation, are we going to be more accepting of murderers,
or are we going to lock them up even more tightly?" asked Jeffrey M. Friedman,
director of the Starr Center for Human Genetics at Rockefeller University. "The
more we find genes that play a role in determining all sorts of attributes, the
more we're going to face these kinds of ethical issues."
Of course, for traits that are socially desirable, people may not be as eager to
accept genetic explanations that seem to trivialize their skills or
accomplishments. When scientists this year found two gene variations that appear
at higher rates in professional dancers than in the general population, many
dancers bristled at the news. In online message boards for the ballet magazine
Pointe, several writers said success in dance was the result of hard work,
passion and good mentors. "Being a dancer requires so much more than what's
there in your body, an emotional strength," said Virginia Johnson, editor of
Pointe and a former principal dancer with the Dance Theater of Harlem.
She paused.
"That genes can't really — well, I guess that's genetic, too, isn't it?"
That
Wild Streak? Maybe It Runs in the Family, NYT, 15.6.2006,
http://www.nytimes.com/2006/06/15/health/15gene.html
Surgeons Work to Separate Twins in L.A.
June 14, 2006
The New York Times
By MARIA NEWMAN
A huge team of doctors at a Los Angeles
hospital began a procedure early this morning to separate a pair of conjoined
twins attached from the chest to the pelvic areas. The operation is expected to
last at least 24 hours.
The complex surgery on Regina and Renata Salinas Fierros began at about 6 a.m.
at the Childrens Hospital Los Angeles. About 80 doctors and staff members will
try to separate many of the girls' vital organs.
The girls, whose parents are from Mexico, are considered ischiopagus tetrapus
twins, which doctors at the hospital said are among the rarest and most complex
to separate because they share many organ systems. The twins are fused on their
front, and today doctors will attempt to separate their liver, intestine,
urinary, reproductive, vascular and musculo-skeletal systems.
"They're attached in a way that even walking across the street would likely be
impossible for them the rest of their lives," the lead surgeon, Dr. James E.
Stein, said at a news briefing on Tuesday. "What we are hoping to do is give
them not just that opportunity but really an opportunity to do everything else
in life that would be considered normal."
A video report from The Associated Press shows the twins a few days ago, two
gurgling dark-haired babies, smiling as they face each other, their little arms
happily flailing about.
The hospital said the girls were born on Aug. 2, 2005, at Los Angeles County-USC
Medical Center. Their parents, Sonia Fierros, 23, and Federico Salinas, 36, are
from Juarez, Mexico. Last spring, when Ms. Fierros was pregnant, she was
hospitalized with a urinary tract infection during a visit to Los Angeles to
visit relatives and learned then that she was carrying conjoined twins.
The couple decided to stay in Los Angeles on an extended tourist visa because
they thought their babies would receive better medical care here, The Associated
Press reported.
Dr. Stein, an attending pediatric surgeon at Childrens Hospital Los Angeles and
an assistant professor of surgery at the Keck School of Medicine of the
University of Southern California, also led the team that successfully separated
conjoined twins in 2003, the hospital said. The hospital said those twins, wards
of the state known publicly as 'Baby A' and 'Baby B', were adopted, along with
their triplet sister, by a "wonderful family and continue to thrive together in
another state."
Today's procedure will likely involve a dozen surgical procedures, Dr. Stein
said.
"The first phase includes dividing the breastbone, liver, intestine, urinary
bladders, genital organs and the bony pelvis," he said. "During the second
phase, the chests, intestines, vaginas, ureters, pelvises and body walls all
will be reconstructed."
Surgeons Work to Separate Twins in L.A., NYT, 14.6.2006,
http://www.nytimes.com/2006/06/14/us/14cnd-twins.html
In Diabetes,
One More Burden for the
Mentally Ill
June 12, 2006
The New York Times
By N. R. KLEINFIELD
Dr. John Newcomer is a psychiatrist who
generally treats people with severe ailments of the mind and spirit. But before
his patients sit down, before he hears about their clammy paranoia or renegade
voices, Dr. Newcomer wants to know about their waist size.
He steers them to a scale to learn their weight. He orders a blood sugar test.
If big numbers come up, he begins a conversation about Type 2 diabetes, a
disease associated with obesity that is appearing with alarming frequency among
the mentally ill.
"Uncontrolled diabetes can ruin a person's life as much as uncontrolled
schizophrenia," said Dr. Newcomer, a professor of psychiatry at Washington
University School of Medicine in St. Louis.
In fact, among the mentally ill, roughly one in every five appear to develop
diabetes — about double the rate of the general population. This is a
little-recognized surge, but one that is jolting mental health professionals
into rethinking how they care for an often neglected population.
For decades, psychiatrists have worried primarily about patients' mental states,
making sure they did no harm to themselves or others because of unrelenting
voices or a smothering depression.
Far more of the mentally ill, however, die today from diabetes and complications
like heart disease than from suicide. Given that mental health specialists are
often the only doctors a mentally ill diabetic ever sees, some have begun to
debate the customary limits of psychiatric practice, deciding to pay much more
attention to physical ailments.
In particular, psychiatrists must confront the fact that diabetes, marked by
dangerously high blood sugar, is often aggravated, if not precipitated, by some
of the very medicines they prescribe: antipsychotic pills that have been linked
to swift weight gain and the illness itself.
"It's bad enough that these people have mental illness, and then they take
treatments and they bring on diabetes," said Dr. Jeffrey Lieberman, chairman of
the psychiatry department at the Columbia University College of Physicians and
Surgeons.
Treating the diabetic mentally ill can be formidable. The regimen of blood
testing, dieting and exercise that controls Type 2 diabetes is often beyond the
attentions of the mentally ill. For patients, the task of taming two
debilitating illnesses can haunt their lives. Michael Schiraldi, 44, a Manhattan
man who has both schizoaffective disease and diabetes, said his mental illness,
now stabilized, was the lesser of his concerns.
"I can't really control the diabetes," he said. "I might die from it."
The doctors who regard diabetes as a galloping threat to the mentally ill
acknowledge that many in their profession still dispute, or ignore, its
consequences. Dr. Newcomer said colleagues often whine about how hard it is to
weigh patients. " 'Oh', they'll say, 'there's no scale' or 'It's in a closet
someplace,' " he said.
Yet he says he hopes other doctors will eventually share his perspective as
diabetes expands among the mentally ill and deepens into an even graver problem.
Betrayals of Body and Mind
Carole Ernst doesn't know how she got diabetes.
Genes? Her mother had it.
Lifestyle? She eats more than she should, exercises less than advisable.
Or was it the pills that shushed the TV?
The TV no longer speaks to her. She stared levelly at the set in her messy room.
It was blessedly quiet.
She is 53 and has battled mental illness since childhood. The pills for her
illness, diagnosed as schizoaffective disorder, have helped. But she feels they
have also made her fat around her abdomen, the kind of fat that can lead to
diabetes.
So even though Ms. Ernst feels better mentally — she no longer imagines everyone
despises her — diabetes has been a crippling insult to her troubled psyche. In
the late hours, alone in her room on the Lower East Side of Manhattan, trapped
in the undertow of two potent diseases, she runs on empty.
"Some nights, the only thing I can do is read my Bible," she said. "I look in
there to find answers. They're hard to find."
Diabetes on top of mental illness asks a lot of a person, and of society. Mental
illness is itself a money sponge, an expense borne largely by tax dollars. But
that cost may be dwarfed by the bill to manage the heart attacks and amputations
that diabetes bestows.
With numerous mental institutions emptied, patients often live in lightly
supervised settings. Many occupy adult homes that struggle, for good reasons and
bad, at providing basic services and are poorly equipped to treat diabetes.
Others live on their own, sometimes in boxes beneath bridges or crumpled in
doorways.
Imagine taking on diabetes if you live alone and find living itself to be a
handful.
"I try not to drink sugared sodas, but sometimes I forget," Ms. Ernst said.
"I'll buy candy — Mary Janes or banana cookies. I know I'm not fooling anybody —
it's my arms and legs they're going to cut off — but sometimes I get the craving
for something sweet."
She sat at a round table in her room, a cool evening of early spring, cradling a
stuffed bunny. She flicked a small smile. "I'm sorry it's not neater," she said,
looking around. "I'm trying."
Ms. Ernst embodies the difficulty of confronting the two diseases with all their
complexities. She takes clozapine for her mind because she can't manage without
it. She has diabetes and can't defeat her weight.
"Disgusting, that clozapine," she said. "Makes you eat everything under the
sun." She takes a lineup of other drugs, too, not all positive for her weight.
She had hit 250, fought her way to 198, and is now at 221.
She lives at Gouverneur Court, a residence run by a nonprofit organization,
where about 15 of the 66 mentally ill residents have diabetes. "Some say they
don't have it, but they do," said Abby Stuthers, the nurse who works there. "Or
they say they have a little diabetes."
Ms. Ernst freely recounts her callused life. Her marriage exploded. Once she was
smacked in the face with a glass ashtray. She opened her mouth — every tooth was
missing.
Now diabetes. Her blood sugar has been O.K., but her vision has worsened. And
she is inconsistent, prey to the fury of her demons.
Susanne Rendeiro, a family nurse practitioner who serves as her primary care
physician, said Ms. Ernst misses half her appointments. Recently, in reviewing
her drugs, Ms. Rendeiro asked about her blood pressure pills. Puzzled, Ms. Ernst
said she was not on blood pressure pills.
Mrs. Rendeiro said she had supposedly been taking them for two years.
"I want to be the best I can be," Ms. Ernst said. "Nobody changes overnight."
Treatment and Cruel Ironies
There was always a lot else wrong with the mentally ill — heart problems and
cancer and H.I.V., as well as diabetes. But for psychiatrists and clinicians it
was enough to worry about mental needs that beggared the imagination.
The spread of diabetes, however, is making the physical conditions impossible to
ignore. "Psychiatrists are literally watching patients balloon up before their
eyes," said Dr. Gail Daumit, an assistant professor of medicine at Johns Hopkins
Medical Institutions.
This has been especially true since the advent of so-called atypical
antipsychotic drugs in the early 1990's. Studies indicate that these drugs can
alter glucose metabolism and stimulate weight gain, particularly in people
predisposed to diabetes.
"Sort of a cruel irony in this," said Dr. Lieberman of Columbia, "is that all of
the drugs do it to some degree, but the ones that have the most effect cause the
most weight gain and metabolic side effects. There's increasing discomfort that
these are driving up deaths and lowering quality of life."
Some cases have been striking: a patient packing on 50 pounds in mere months,
for example. Diabetes arrived as quickly, and sometimes subsided if the drugs
were halted. In certain instances, there was no weight gain, but still diabetes
came, often in patients who were already heavy. Studies have indicated that
dozens of these patients died from diabetes-related complications.
The Food and Drug Administration requires atypical antipsychotics to bear
warning labels about diabetes risk, though drug makers say patients taking them
who develop diabetes were destined to get it anyway.
Robin Stigliano's psychiatrist has her taking Haldol by injection as well as one
of the drugs most closely associated with weight gain, Zyprexa. They have helped
her schizophrenia, but Ms. Stigliano, 37, who lives in a Brooklyn adult home,
has seen her weight soar to 241 pounds from 150. And when she gets her Haldol
infusion every three weeks, all she wants to do is sleep. "It's my favorite
activity," she said.
Without the drugs, psychiatrists believe, many high-functioning patients would
find themselves in institutions or jail. "These drugs are enormously
beneficial," said Dr. P. Murali Doraiswamy, head of biological psychiatry at
Duke University. "But they have an Achilles heel."
A few years ago, Dr. Doraiswamy reported a case of a mentally ill person who got
diabetes and was prescribed insulin. The impact of having two serious conditions
overwhelmed him. He wound up trying to kill himself by insulin overdose.
Some researchers think it is possible the rash of diabetes stems in part from
mental illness itself. Studies associate the onset of diabetes with depression.
The mentally ill are also at high risk because they tend to eat poorly, get
little exercise and have limited access to health care.
In a 2003 survey, the city's health department found that about 17 percent of
adults who reported symptoms of a mental illness, or 52,000, have diagnosed
diabetes. Elsewhere, rates are as great or greater. Even these estimates may be
low, experts said, because the mentally ill see doctors sporadically and their
illnesses may be underdiagnosed.
The rates of diabetes and obesity are nudging Dr. Doraiswamy and others in his
field — in modest ways thus far — toward prevention, toward screening people for
diabetes before choosing drugs and connecting better with primary care doctors.
"This wouldn't be a big problem if most mentally ill patients had a primary care
provider, but they don't," said Dr. Newcomer at Washington University. "And it's
never been part of the game plan for the psychiatrist to write the prescription
for your blood pressure medicine or your diabetes medicine."
He feels change is imperative. "The days when I don't do windows can't go on,"
he said.
Dr. Kenneth Duckworth, medical director for the National Alliance on Mental
Illness, agreed. "I think the field has been passive," he said. "We viewed it
that we do symptoms and you run your life."
Stimulating change is not easy. Psychiatrists have a problem simply getting
patients to stay on their drugs. Resources are inadequate.
"Psychiatry is historically a couch and the chair," Dr. Duckworth said. "How do
you get movement into the equation?"
He said that he weighed his patients, checked sugars. But few psychiatrists are
set up to do this. Treating diabetes, they say, was not what they were trained
to do. And where, they ask, do they find time in 15-minute appointments?
"Most psychiatrists barely look at their patients," said Dr. Donna Ames
Wirshing, a staff psychiatrist at the West Los Angeles Veterans Administration
Medical Center. She recently asked 30 how many weighed their patients; 3 hands
went up.
Dr. Wirshing and her husband, Dr. William Wirshing, are experimenting with the
use of nutrition and exercise coaches for mentally ill patients.
Couches could be replaced with exercise bikes. Or, as Dr. David Hellerstein,
associate professor of clinical psychiatry at Columbia's College of Physicians
and Surgeons, noted, "Instead of having the patient lie down and you say, 'So
tell me why you fight with your brother,' you could say to the patient, 'Let's
take a walk around the block while you tell me about why you fight with your
brother.' "
For the most part, however, psychiatrists confront the knotty questions without
ready answers.
If some 10 percent of schizophrenics kill themselves, and clozapine is the only
antipsychotic medication demonstrated to significantly reduce suicide, but it
has grave side effects, like its association with diabetes, is it miracle or
monster? Or both?
"When I chat with patients, about clozapine, I say, 'This may give you your mind
back, but it may hurt your body,' " Dr. Duckworth said. "I think of it as
psychiatric chemotherapy. Your hair won't fall out, but you may get diabetes."
How do patients respond? "Some say, 'If this will give me my mind, I'll take
anything,' " he said. "Some say, 'There's nothing wrong with me, why are we even
having this conversation?' About 60 percent of schizophrenics don't recognize
that they have it. There are very few easy answers in my line of work."
Housing the Ill and Diabetic
Surf Manor squats on the tip of Coney Island, one of the dozens of profit-making
adult homes in the city where thousands of the mentally ill live. Residents
complain about the food. Activities are light on exertion. The week's offerings
are taped to the wall: dominoes, blackjack, manicures, jewelry class.
So the men and women eat, sleep, smoke, watch TV, sleep — then do it all over
again. Unsurprisingly, those who live there say, dozens of the 200 residents
struggle with diabetes.
These often-troubled homes where so many of the mentally ill are housed,
frequently grumbling about inadequate attention to their needs and their
dignity, can be hideously difficult places for someone at high risk for
diabetes. And that is basically everyone who lives there.
Leslie Hinden, a chatty man of 51, sat listlessly in the lounge, near the junk
food dispensers. He'd be buying sweets but was broke from binging.
He has had schizoaffective disease — characterized by symptoms of schizophrenia
and depression — for most of his life. Sometimes he hears Indian war whoops in
his head. About 17 years ago, he picked up diabetes, too.
His blood sugar was 289 that morning, he said. A normal fasting blood sugar
reading is below 126 milligrams per deciliter.
"I cheated," he said. "Last night I ate two eclairs. Had a Coke. A lot of times
I don't cheat and it goes up to 300. I don't know what to do."
Why the binge last night?
"I don't know," he said. "I felt scared."
A recent State Department of Health sampling of 19 homes found that nearly a
quarter of residents had diabetes. The homes say they do what they can. Some
have diabetes sections in the dining halls, where occupants get a sugar-free
dessert.
"I'm not a doctor, but we're very helpful," said Mordechai Deutscher, the case
manager at Surf Manor, who said he did not think the home had many diabetics.
"The people here are doing very well."
Even mental health advocates have not given diabetes much attention. The
Commission on Quality of Care and Advocacy for Persons with Disabilities, a
state watchdog agency, said it has never examined diabetes prevalence or care.
At Surf Manor, Mr. Hinden, like the other diabetic residents, cannot have a
blood sugar meter or give himself insulin. Needles are considered perilous. He
depends on the staff. But no one prescribes motivation or understanding. And
where diabetes requires vigilant self-management, illnesses like schizophrenia
often mean memory problems and lack of drive.
"I'll be honest with you, I don't understand diabetes," Mr. Hinden said. "I
don't understand it at all."
Joseph Franklin, 47, sat down, all 300-plus pounds of him. He said he has been
taking diabetes drugs for seven years. "It's just in case," he said.
He said he was bipolar: "I couldn't see people with shoes on. If I saw someone
with shoes on, it could do something to my forehead."
He spread out some greeting cards he had made. He leaned close. "Listen, I don't
want everyone to hear this," he said, "but it's very possible that, unless the
doctor made a mistake, I do have diabetes."
A stoic man of great girth named Lee Symons, 57, nodded. He had it, too. He
hears guitars and banjos thrumming in his head.
Was he trying to diet?
"No one told me to," he murmured.
What about the diabetes?
"As long as it doesn't hurt, I don't mind it," he said. "It's just diabetes."
In
Diabetes, One More Burden for the Mentally Ill, NYT, 12.6.2006,
http://www.nytimes.com/2006/06/12/health/12diabetes.html
U.S. Approves Use of Vaccine for Cervical
Cancer
June 9, 2006
The New York Times
By GARDINER HARRIS
WASHINGTON, June 8 — Federal drug officials on
Thursday announced the approval of a vaccine against cervical cancer that could
eventually save thousands of lives each year in the United States and hundreds
of thousands in the rest of the world.
The vaccine, called Gardasil, guards against cancer and genital warts caused by
the human papillomavirus, the most common sexually transmitted disease. It is
the culmination of a 15-year effort that began at the National Cancer Institute
and a research center in Australia, and health officials described the vaccine
as a landmark.
Federal vaccine experts are widely expected to recommend that all 11- to
12-year-old girls get the vaccine, but its reach could be limited by its high
price and religious objections to its use.
Merck, Gardasil's maker, said a full, three-shot course would cost $360, making
Gardasil among the most expensive vaccines ever made.
"This is a huge advance," said Dr. Jesse Goodman, director of the Food and Drug
Administration's biologics center. "It demonstrates that vaccines can work
beyond childhood diseases to protect the health of adults."
The vaccine prevents lasting infections with two human papillomavirus strains
that cause 70 percent of cancers and another two strains that cause 90 percent
of genital warts. But if girls have already been exposed to those strains, the
vaccine has no effect, so health experts want the vaccine given before girls
have sex. The median age at which girls have sex is 15.
A Merck spokeswoman said Gardasil, which was approved for girls and women ages 9
to 26, would be available in doctors' offices by the end of June.
The vaccine is not approved for use in boys, although Merck hopes one day to
change that. If the company is successful, analysts expect that sales could
surpass $4 billion by 2010.
Cervical cancer is the second-leading cause of death in women across the globe,
affecting an estimated 470,000 women and killing 233,000 each year. Widespread
use of Pap smears has reduced its toll in richer nations. In the United States,
about 9,710 women contract cervical cancer each year, and some 3,700 die.
Private health insurers are likely to cover the vaccine for 11- and 12-year-old
girls, although older women may have to pay for it themselves.
Vaccines are one of the most cost-effective medical interventions available. But
Gardasil's price could put it out of reach for most women in poor countries and
some in the United States who lack private insurance.
A federal program is expected to provide the vaccine to 45 percent of the
children in the United States for whom it is recommended. But state programs
that cover other children are having trouble buying other expensive vaccines.
North Carolina, for instance, spends $11 million annually to provide every child
with seven vaccines. Gardasil alone would probably cost at least another $10
million.
"Increasingly, states are asked to make a Sophie's choice about which diseases
they will allow children to be hospitalized or killed by," said Dr. Paul Offit,
director of infectious diseases at Children's Hospital of Philadelphia.
Liberals in Congress and elsewhere have warned that the Bush administration and
religious groups should not interfere with Gardasil's approval or required
use.In response, many conservative groups have made statements supporting the
vaccine.
"Despite rumors to the contrary, our organization doesn't oppose the vaccine and
we have taken no position regarding mandatory laws," said Wendy Wright,
president of Concerned Women of America, a conservative group based in
Washington.
Some groups support the vaccine but oppose mandatory vaccinations because
cervical cancer is caused by a sexually transmitted virus.
"We can prevent it by the best public health method, and that's not having sex
before marriage," said Linda Klepacki of Focus on the Family, a Christian
advocacy organization based in Colorado Springs.
But scientific and budgetary issues are much more likely to determine Gardasil's
uptake. Three shots must be given over six months. Such a schedule is routine
among infants, but preteens are tougher to corral into doctors' offices.
An independent panel formed by the Centers for Disease Control and Prevention is
scheduled to decide June 29 who should get the vaccine.
The panel is expected to recommend vaccinations for all 11- to 12-year-old
girls, while agreeing that girls as young as 9 or women as old as 26 can get the
vaccine if they wish. It is also expected to suggest that states make
vaccinations mandatory.
Many states will not have the money to do much more, said Dr. Leah Devlin, state
health director for North Carolina and president of the Association of State and
Territorial Health Officials.
Already, North Carolina has been unable to provide six federally recommended
vaccines to all children because of cost, Dr. Devlin said. The state cannot
mandate any vaccine that it does not agree to provide.
In the United States, about 20 million people are infected by the human
papillomavirus each year. By the time women reach the age of 50, 80 percent have
been infected.
Most infections are quickly dealt with by the immune system. But some strains
cause changes in cells that line the cervix in some women. The changes years
later can turn into cancer. Most patients contract the disease in their 40's and
50's.
GlaxoSmithKline, based in London, is also developing a vaccine against cervical
cancer that it expects to submit for F.D.A. approval at the end of the year.
Pap smears can detect precancerous changes to the uterus, but the tests are
sometimes wrong, missing some cases and leading to unnecessary procedures in
others. Because Gardasil protects against only four viral strains and its
effects in those four will take decades to have widespread effect, health
officials are recommending that women continue to undergo routine Pap tests.
Silvia Ford, a 35-year-old stay-at-home mother from Maryland, learned in
November 2004, just three months after bearing her second child, that she had
cervical cancer. Surgeons removed her uterus, for which she has no regrets. "I
wanted to be around to take care of the two children I've already got," she
said.
Ms. Ford is checked every three months for signs of cancer. She plans to have
her daughter, now 6, vaccinated at some point.
"This vaccine should not lead to an argument about when girls have sex," Ms.
Ford said. "It's about saving the lives of women in their child-bearing years,
letting them have children or take care of the children they already have."
Merck had originally hoped to get the vaccine approved for use in boys. But
although women have routinely allowed swabs to be taken of their vaginal cells,
the company found that men rebelled against the use of emery boards to collect
cells from their penises. Researchers eventually discovered that jeweler's-grade
emery paper effectively removed cells without alarming men and were able to
complete their studies.
U.S.
Approves Use of Vaccine for Cervical Cancer, NYT, 9.6.2006,
http://www.nytimes.com/2006/06/09/health/09vaccine.html
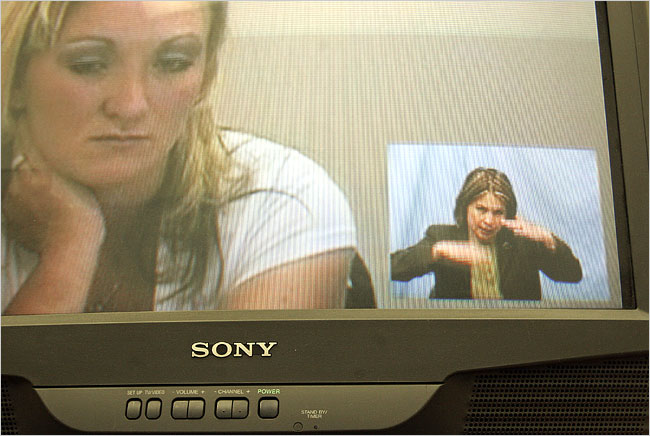
Dr. Sara Gibson, right, with a patient who asked to be
identified only as C.
They say they sometimes forget they are not in the same
room.
Jeff Topping for The New York Times
June 8, 2006
TV Screen, Not Couch, Is Required for
This Session NYT
8.6.2006
http://www.nytimes.com/2006/06/08/us/08teleshrink.html
TV Screen, Not Couch,
Is Required for This
Session
June 8, 2006
The New York Times
By KIRK JOHNSON
FLAGSTAFF, Ariz. — Dr. Sara Gibson looked into the
television screen and got right down to it.
"What's keeping you alive at this point?" she asked her patient, a middle-aged
woman who asked to be identified only as D. D grimaced, looked down, then to the
side and finally into Dr. Gibson's face, which filled the screen before her in a
tiny clinic three hours east of here in the Arizona desert.
"Nothing," said D, who Dr. Gibson says suffers from bipolar disorder and
post-traumatic stress from the sexual abuse she suffered as a child.
It is Wednesday in the hinterlands of rural Arizona, and the psychiatrist is in.
Sort of.
Actually, Dr. Gibson was here in Flagstaff in a closet-size office of a
nonprofit medical group, with a pale blue sheet behind her as a backdrop and a
cup of tea at her side. She is one of a growing number of psychiatrists
practicing through the airwaves and wires of telemedicine, as remote doctoring
is known.
Psychiatry, especially in rural swaths of the nation that also often have deep
social problems like poverty and drug abuse, is emerging as one of the most
promising expressions of telemedicine. At least 18 states, up from only a
handful a few years ago, now pay for some telemedicine care under their Medicaid
programs, and at least eight specifically include psychiatry, according to the
National Association of State Medicaid Directors. Six states, including
California, require private insurers to reimburse patients for telepsychiatry,
according to the National Conference of State Legislatures.
Growing prison populations have a lot to do with the trend. Since reimbursement
for prison care is easy and safety issues for doctors are significant, many
telemedicine programs, notably an ambitious one in Texas, started there. Now,
the falling price of technology is making care available to far-flung rural
residents like D.
Dr. Gibson rides a disembodied circuit through this terrain. On Wednesdays, she
sees patients in the tiny community of Springerville near the New Mexico border
through a firewalled T1 data line, and on Thursdays in St. Johns. Each side of
the exchange has its own television-mounted camera, angled so that doctor and
patient can maintain the illusion of looking into each other's eyes in real
time.
And so, through illusion and delusion, depression, anxiety, paranoia — and here
and there a laugh or two — a day in the life of a rural telepsychiatrist and her
patients unfolded.
"Is there self-harm going on, too?" Dr. Gibson pressed D, typing notes into the
computer and glancing back at the screen. D paused, then quietly said, "Yeah."
Dr. Gibson, 44, was a pioneer in the field. She has been seeing patients only
this way for 10 years and is still one of a handful of doctors in the country
who practice telepsychiatry exclusively. Her territory is Apache County, which
is about the size of Massachusetts and Connecticut combined, but which lacks
even a single psychiatrist on the ground for its 69,000 residents despite
widespread problems of poverty, drug use, child abuse and a suicide rate that is
twice the national average.
The American Psychiatric Association says on its Web site that it supports
telemedicine, "to the extent that its use is in the best interest of the
patient," and practitioners meet the rules about ethics and confidentiality. But
in places like Apache County, where the alternative is no treatment at all, most
mental health workers say that every new wire and screen is to be deeply
cheered.
"Basically, doctors can do, surprisingly, almost everything," said Don McBeath,
the director of telemedicine and rural health at the Texas Tech University
Health Sciences Center in Lubbock. "The difference is they can't touch you or
smell you."
Dr. Gibson said the lack of smelling and touching, at least when it comes to
psychiatry, has proved to be a good thing. Being physically in the presence of
another human being, she said, can be overwhelming, with an avalanche of sensory
data that can distract patient and doctor alike without either being aware of
it.
"Initially we all said, 'Well, of course it would be better to be there in
person,' " she said. "But some people with trauma, or who have been abused, are
actually more comfortable. I'm less intimidating at a distance."
Some of the doctor's patients, who agreed to allow a reporter and photographer
to observe their therapy sessions over two recent days — one day in Flagstaff
with Dr. Gibson, the second day in a field clinic in St. Johns, population 3,000
— said they were in fact perfectly happy with the doctor's being hundreds of
miles away, though some were quick to add that no offense was intended.
"Some people don't want to have to deal with a real person," said one patient, a
63-year-old woman who has dementia and bipolar disorder.
One thing Dr. Gibson has learned over the years is that she should not wear
stripes or zigzag patterns, which can look strange on television, especially to
already disturbed people. For patients with paranoia, she regularly pans the
camera around her little room to prove that no one else is lurking and
listening. (A white-noise machine purrs outside Dr. Gibson's office door, muting
the exchanges within, and no session is ever recorded.)
She worries, sometimes, about the children she sees, almost all of whom
immediately and enthusiastically embrace the idea of a talking to the nice,
chatty woman on the television. "Do they understand that the TV doesn't always
talk to them?" Dr. Gibson said.
Another patient, Mike Kueneman, who allowed his full name to be used, has seen
Dr. Gibson for about five years, through the periods with the voices in his head
and what he calls the "psychotic episode" that landed him in jail this year on
burglary charges. Mr. Kueneman said he felt more comfortable with Dr. Gibson,
even though they have never met in person, than he does with most of the people
he knows.
Like most of Dr. Gibson's patients, he pays little or nothing to see her. State
programs for low-income and mentally ill people pay for the $120 psychiatric
evaluations and $40 follow-up visits — and for the medicines she prescribes,
which can cost thousands of dollars.
"It's hard for me to trust any other doctor," said Mr. Kueneman, who attended a
telesession in the St. Johns clinic in leg shackles and handcuffs, accompanied
by an Apache County sheriff's deputy.
Some things did not happen as expected. Dr. Gibson predicted, for example, that
at least one patient would incorporate the teleconferencing technology into his
or her delusions and come to believe that telemedicine could be used to read
people's thoughts or get inside their heads.
To the contrary, in matters of the psyche — two people in two rooms looking at
each other across a cool electronic medium — it is still all about human
connection.
"I just feel like she's here," said a 24-year-old mother of three who asked to
be referred to as C. C was struggling with depression, anxiety and fantasies of
suicide. "I sometimes forget we're not in the same room."
Dr. Gibson spoke up from her room in Flagstaff: "That's funny, I would say that
I feel the same way."
Dr. Gibson and C have known each other across the telewaves since C became a
single mother on her own at age 17.
The emotions ran deep as they spoke and C described the dark thoughts that
sometimes come at night. Gripped by insomnia, convinced that someone else is in
the trailer she lives in, her mind races, she said, and the fantasy rolls out of
how she might take her youngest child with her and disappear, driving off into
the night.
"I don't want you killing yourself," Dr. Gibson said with a matter-of-fact tone.
"So that means talking."
Apache County had a genuine, in-the-flesh psychiatrist once, Dr. Julia Martin,
who practiced there for about 10 years until her retirement in 1996.
Dr. Martin was trained as a pediatrician and went back to school for psychiatry
in her 50's. For more than a decade, she was it, the county's solo psychiatrist
and also the only one serving the nearby Fort Apache Indian Reservation.
"You did get to know your patients pretty well — sometimes better than you'd
like," Dr. Martin, 74, said in a telephone interview from her home in a remote
corner of the county. Sometimes people would show up in the middle of the night,
she said, desperate to see her. Other times, they delivered brownies.
What Dr. Gibson's patients imagine of her life and what she is like when she is
not on camera is unknown. She sometimes mentions her children to them, and her
passions for music and singing. She speculated that telemedicine has probably in
some ways amplified and enlarged her image in the minds of some patients — that
if she is on television she must be really important, larger than life.
She has been to Apache County once, for a "meet the psychiatrist" event in St.
Johns years ago. Many of the patients who showed up remarked, she said, about
how much shorter she was than they had expected.
TV Screen, Not
Couch, Is Required for This Session, NYT, 8.6.2006,
http://www.nytimes.com/2006/06/08/us/08teleshrink.html
Use of Antipsychotics by the Young
Rose Fivefold
June 6, 2006
The New York Times
By BENEDICT CAREY
The use of potent antipsychotic drugs to treat children and
adolescents for problems like aggression and mood swings increased more than
fivefold from 1993 to 2002, researchers reported yesterday.
The researchers, who analyzed data from a national survey of doctors' office
visits, found that antipsychotic medications were prescribed to 1,438 per
100,000 children and adolescents in 2002, up from 275 per 100,000 in the
two-year period from 1993 to 1995.
The findings augment earlier studies that have documented a sharp rise over the
last decade in the prescription of psychiatric drugs for children, including
antipsychotics, stimulants like Ritalin and antidepressants, whose sales have
slipped only recently. But the new study is the most comprehensive to examine
the increase in prescriptions for antipsychotics.
The explosion in the use of drugs, some experts said, can be traced in part to
the growing number of children and adolescents whose problems are given
psychiatric labels once reserved for adults and to doctors' increasing comfort
with a newer generation of drugs for psychosis.
Shrinking access to long-term psychotherapy and hospital care may also play a
role, the experts said.
The findings, published yesterday in Archives of General Psychiatry, are likely
to inflame a continuing debate about the risks of using psychiatric medication
in children. In recent years, antidepressants have been linked to an increase in
suicidal thinking or behavior in some minors, and reports have suggested that
stimulant drugs like Ritalin may exacerbate underlying heart problems.
Antipsychotic drugs also carry risks: Researchers have found that many of the
drugs can cause rapid weight gain and blood lipid changes that increase the risk
of diabetes. None of the most commonly prescribed antipsychotics is approved for
use in children, although doctors can prescribe any medication that has been
approved for use.
Experts said that little was known about the use of antipsychotics in minors:
only a handful of small studies have been done in children and adolescents.
"We are using these medications and don't know how they work, if they work, or
at what cost," said Dr. John March, a professor of child and adolescent
psychiatry at Duke University. "It amounts to a huge experiment with the lives
of American kids, and what it tells us is that we've got to do something other
than we're doing now" to assess the drugs' overall impact.
But many child psychiatrists say that antipsychotic medication is the best
therapy available for children in urgent need of help who do not respond well to
other treatments. Without them, they say, many unpredictable, emotionally
unstable children would end up institutionalized.
Dr. Mark Olfson, a professor of clinical psychiatry at Columbia University and
the lead author of the study, financed in part by the National Institute of
Mental Health, said the popularity of antipsychotic drugs might result in part
from "the fact that psychiatrists have few other pharmacological options in
certain patients."
The study, which looked at visits to pediatricians and other doctors, found that
psychiatrists were the most likely to prescribe antipsychotic drugs.
In light of how little these drugs have been studied in children, Dr. Olfson
said, "to me the most striking thing was that nearly one in five psychiatric
visits for young people included a prescription for antipsychotics."
The Columbia investigators analyzed data from the National Center for Health
Statistics survey of office visits, which focuses on doctors in private or group
practices. They calculated the number of visits in which an antipsychotic drug
was prescribed to people under the age of 21 and collected information on
patients' medical histories. The total number of visits that resulted in
prescriptions for the drugs increased to 1,224,000 in 2002 from 201,000 1993 to
1995.
The researchers attributed some of the increase to the availability of a new
class of drugs for psychosis, called atypical antipsychotics, that were
introduced in the early and mid-1990's.
The newer drugs, heavily marketed by their makers, were attractive in part
because they appeared less likely than older types of antipsychotics to cause
side effects like tardive dyskinesia, a neurological movement disorder similar
to Parkinson's disease.
From 2000 to 2002, the new study found, more than 90 percent of the
prescriptions analyzed were for the newer medications, and most of the patients
were boys, predominantly Caucasian children, who were significantly more likely
to see psychiatrists than other ethnic groups.
Some experts also pointed to an increase in the diagnosis of bipolar disorder in
children as a contributing factor. In recent years, psychiatrists have begun to
diagnose the disorder in extremely agitated, often aggressive children with mood
swings — short surges of grandiosity or irritation that alternate with periods
of despair. These symptoms in children are thought to be related to the classic
euphoria and depressions of adult bipolar disorder.
At the same time, several of the atypical antipsychotics, including Risperdal
from Janssen and Zyprexa from Eli Lilly, won approval for the treatment of mania
in adults.
Some psychiatrists now routinely prescribe atypical antipsychotics "off label"
for young people thought to have bipolar disorder, and researchers have begun to
study the drugs in children as young as preschool age.
In the new study, about a third of the children who received antipsychotics had
behavior disorders, which included attention deficit problems; a third had
psychotic symptoms or developmental problems; and another third were suffering
from mood disorders. Over all, more than 40 percent of the children were also
taking at least one other psychiatric medication.
"We feel the medications are effective in children with bipolar and have some
data to show that," said Dr. Melissa DelBello, an associate professor of
psychiatry at the University of Cincinnati, who has done several studies of the
drugs.
Dr. DelBello said that the field "desperately needs more research" to clarify
the effects of the antipsychotic drugs but that many children struggling with
bipolar disorder got more symptom relief on these drugs than on others, allowing
psychiatrists to cut down on the overall number of medications a child is
taking.
Lisa Pedersen of Dallas, the mother of a 17-year-old boy being treated for
bipolar disorder, said he was unpredictable, hostile and suicidal before
psychiatrists found an effective cocktail of drugs, which includes a daily dose
of antipsychotic medication.
"Believe me, I would never choose having him on these meds," Ms. Pedersen said
in a telephone interview. "It's not fun watching a child deal with the side
effects. But finding the right combination of medicine has made his life worth
living."
Yet this process is one of trial and error for many children. Ms. Pedersen said
her son had responded badly to the first two antipsychotic drugs he received.
And some experts think the way that psychiatric drugs are prescribed is
obscuring any understanding of underlying disorders and the optimal treatments.
"If you're going to put children on three or four different drugs, now you've
got a potpourri of target symptoms and side effects," said Dr. Julie Magno Zito,
an associate professor of pharmacy and medicine at the University of Maryland.
Dr. Zito added, "How do you even know who the kid is anymore?"
Use of
Antipsychotics by the Young Rose Fivefold, NYT, 6.6.2006,
http://www.nytimes.com/2006/06/06/health/06psych.html
2 New Efforts to Develop Stem Cell Line for Study
June 7, 2006
The New York Times
By NICHOLAS WADE
Scientists at two universities — Harvard and the University
of California, San Francisco — will try to develop embryonic stem cells from the
adult cells of patients suffering from certain diseases.
Their purposes in creating the cell lines, which require making an early human
embryo, are to study how the diseases develop and also to see if replacement
cells can be generated to repair the patient's own degenerating tissues. But the
field, despite its much emphasized promise, faces many serious uncertainties.
"Clinical applications may be a decade or more away," said George Q. Daley, a
Harvard expert on blood diseases.
Harvard announced its plans yesterday at a news conference; the University of
California, San Francisco, did so less conspicuously a month ago, resuming a
program abandoned in 2001. Both universities, having received required
approvals, will at first obtain the human eggs needed for cloning from fertility
clinics, starting with eggs deemed too low quality to produce a successful
pregnancy. Both programs are privately financed because federal support for
human stem cell research is available only for cell lines made before August 9,
2001.
Advanced Cell Technology in Worcester, Mass., also has a human nuclear transfer
program "well under way," said Robert Lanza, the company's vice president, but
has run into problems in recruiting egg donors. Under guidelines issued by the
National Academy of Sciences, which are voluntary but widely observed, donors
may not be paid anything beyond expenses.
The new efforts, if successful, would accomplish what the disgraced South Korean
scientist Woo-Suk Hwang claimed he had achieved in articles published in Science
in 2004 and 2005. Both papers turned out to be based on forged data. But the
flaws remained undetected by scientists involved in the cloning field, raising
doubts about the rigor and expertise with which the new field was being
conducted. The problems came to light not through criticism by scientific peers,
but only after a whistle-blower in Dr. Hwang's lab contacted a Seoul television
station.
The University of California, San Francisco, said last month that one of its
researchers, Renee Reijo Pera, would start the cloning procedure, which involves
transferring the nucleus of an adult cell into an unfertilized egg whose own
nucleus has been removed.
A composite egg of this kind should develop in glassware into an early embryo,
or blastocyst, from which embryonic stem cells could be isolated. There is no
evident reason why this should not work in people as it has already done in
several animal species, yet so far no one has succeeded. Dr. Hwang used no less
than 2,000 fresh eggs donated by a healthy women but failed to accomplish
anything useful.
Dr. Reijo Pera will switch to using donated eggs if those rejected by fertility
clinics do not work, a university spokeswoman said. Harvard researchers said
yesterday that they too would seek to derive eggs from healthy donors in the
future.
Dr. Lanza, of Advanced Cell Technology, said that freshly harvested human eggs
were "much better" for nuclear transfer experiments but that a six-month
campaign by his company to recruit donors "appears to be a losing effort."
Many women had come forward, saying they would donate their eggs for research
without compensation but, after seeing the battery of tests required, "most of
the donors change their mind once they realize what's involved," Dr. Lanza said.
If research should establish that replacement tissues can be developed for a
patient through the nuclear transfer technique, probably tens or hundreds of
donated human eggs would be needed for each operation. Some scientists regard
such a requirement as impractical, arguing that researchers should learn how to
reprogram an adult cell's nucleus back to embryonic state without the use of
human eggs. But this requires a far deeper understanding of human cells than is
yet at hand.
Three Harvard scientists described their proposed research yesterday, promising
not to discuss it further in public until they had firm results ready to be
published. Dr. Daley hopes to develop, via nuclear transfer, embryonic stem
cells from patients with blood diseases. He will try to correct the genetic
defect behind the disease, then develop blood stem cells that could be engrafted
in the patient's marrow.
The two other scientists, Douglas Melton and Kevin Eggan, said they would
develop embryonic stem cell lines from diabetic patients, hoping to understand
the development of the disease from its earliest moments at the cellular level.
2 New Efforts to
Develop Stem Cell Line for Study, NYT, 7.6.2006,
http://www.nytimes.com/2006/06/07/science/07stem.html
Racial Component Is Found in Lethal Breast Cancer
June 7, 2006
The New York Times
By DENISE GRADY
Young black women with breast cancer are more prone than
whites or older blacks to develop a type of tumor with genetic traits that make
it especially deadly and hard to treat, a study has found.
Among premenopausal black women with breast cancer, 39 percent had the more
dangerous kind, called a "basal like" subtype, compared with only 14 percent of
older black women and 16 percent of nonblack women of any age. Researchers are
not sure why.
The study, being published today in The Journal of the American Medical
Association, is the first to measure how common the different genetic subtypes
of breast tumors are in American women, and to sort the subtypes by race. The
authors said more research was needed to test their conclusions.
The finding has no immediate effect on treatment, because there is no treatment
that specifically concentrates on basal-like cancer. But scientists are trying
to create drugs that will zero in on it.
The study helps explain something that was already known: although breast cancer
is less common in blacks than whites, when black women do develop the disease,
they are more likely to die from it, especially if they are under 50. Among
those younger women, the breast cancer death rate in blacks is 11 per 100,000,
compared with only 6.3 in whites.
The new data about tumor types is not the whole story, researchers say, because
some of the disparity may also result from a lack of access to health care among
blacks or differences in nutrition, personal habits or environmental exposures.
The genetic discovery is "somewhat alarming," but also a "good thing," because
it exposes details about the cancer that should help doctors identify specific
drugs to fight it, said the study's main author, Dr. Lisa A. Carey, the medical
director of the University of North Carolina-Lineberger breast center.
Several research groups including her own have already begun testing new drugs
against this type of breast cancer, Dr. Carey said. The work involves finding
drugs to block specific molecules that these tumors need to grow. If the trials
succeed, new treatments could be available within a few years, perhaps even as
soon as a year from now, she predicted.
These tumors are identified not by looking through a microscope, but by special
tests that measure patterns of genetic activity.
"Things that to my eye and a pathologist's eye look similar turn out to be
biologically very different," Dr. Carey said, adding that the tests were now
strictly a research tool and were not done routinely in women with breast
cancer.
Dr. Larry Norton, a breast cancer expert at Memorial Sloan-Kettering Cancer
Center in New York who was not part of the study, said the research was
extremely well done and important. He said there was preliminary evidence from
other studies that basal-like tumors were the most common kind found in Africa,
and that understanding what caused them could help point the way toward better
treatments and methods of prevention.
Dr. Olufunmilayo Olopade, director of the center for clinical cancer genetics at
the University of Chicago, said she had found high rates of basal-like tumors in
young women in Nigeria and Senegal, most of whom died. In many, the disease ran
in their families.
The work has not yet been published, but Dr. Olopade said the message to black
women, and to women of all races, was that if their mothers, sisters or
daughters developed breast cancer at an early age, they needed to start
screening for it well before age 40, to seek genetic counseling and to consider
preventive drugs and perhaps preventive surgery if they proved to be at high
risk.
Basal-like tumors tend to grow fast and spread quickly, and they are more likely
than other types to be fatal. They are not fed by the hormone estrogen, and so
cannot be treated or prevented with estrogen-blocking drugs like tamoxifen or
raloxifene. Herceptin, another breast cancer drug, is also useless against these
tumors. The tumors are not stimulated by the hormone progesterone, either. For
that reason, cancer specialists call them "triple negative."
Standard chemotherapy does help, and women with basal-like tumors benefit more
from it than women with other breast cancers. But even with treatment, those
with basal-like tumors are less likely to survive.
Women with mutations in a gene called Brca1 tend to develop this kind of
aggressive breast tumor. In the past, researchers thought Brca1 mutations did
not occur in black women, but Dr. Olopade dismissed that notion as a myth,
saying the mutations were found just as often in black women as in other
populations. She and Dr. Carey said other mutations, not yet discovered, might
also predispose black women to the basal-like tumors.
Dr. Carey's research was based on stored tissue samples from 496 women who had
breast cancer diagnoses from 1993 to 1996 and who were included in a project
called the Carolina Breast Cancer Study. Their average age was 50, and 40
percent identified their race as African-American.
The researchers used new techniques of molecular biology to find patterns of
gene activity in the cancer cells, to classify the tumors accordingly and then
to sort the genetic subtypes by race, menopausal status, other tumor traits and
survival.
"The same technology that identified the subtypes also tells us about the
biology of the subtypes," Dr. Carey said. "Once you know what makes it tick, you
can figure out how to stop the ticking. It's opened up a window on it."
The goal is to find particular molecules in a cell that drive proliferation or
tumor survival, and to block them.
"If it looks like a particular cancer cell is dependent on a certain pathway to
live or grow, and if you can shut it down preferentially in that cancer cell,
you can stop it," Dr. Carey said.
Newer cancer drugs like herceptin and Gleevec, which is used for certain types
of leukemia and gastrointestinal tumors, work in this so-called targeted
fashion, and so does Tykerb, a new breast cancer drug described last weekend at
a meeting of the American Society for Clinical Oncology. For certain cancers,
targeted treatments are far more effective than standard chemotherapy, more of a
buckshot approach.
Breast cancer experts hope to find better treatments than chemotherapy for many
types of the cancer, and Dr. Carey said, "That's the challenge, getting away
from chemo for this subtype."
The next step in the research is to look for risk factors for the basal-like
subtype, in hopes of finding ways to prevent it, she said.
"There's a lot of smart people working very hard on this," Dr. Carey said. "I'm
very optimistic."
Racial Component
Is Found in Lethal Breast Cancer, NYT, 7.6.2006,
http://www.nytimes.com/2006/06/07/health/07breast.html
In State Races,
Tough Questions About Abortion
June 5, 2006
The New York Times
By MONICA DAVEY
IOWA CITY, June 2 — Even in a room of sixth graders sitting
cross-legged on the floor, usually the safest of venues for political
candidates, the question emerged from one sweet face: What is your position on
abortion?
Mike Blouin, who is running for governor, has been asked that a lot lately,
though abortion bans are more typically the purview of presidents who might pick
United States Supreme Court nominees or senators who might confirm them. The
Supreme Court declared a constitutional right to abortion 33 years ago in Roe v.
Wade.
But with South Dakota this year having passed the country's most restrictive
state abortion law in decades and a sense among some advocates on both sides of
the abortion debate that a changed Supreme Court could one day leave the
abortion question in the hands of the states, tough questions about abortion
rights are being raised in local races across the country.
Questions about how to regulate or restrict abortion have long been issues in
state races. But in campaigns for governor and the Legislature here in Iowa and
in numerous other states, many candidates are being asked not only about limits
on abortion, but also a far broader, starker question: to outlaw or not to
outlaw?
"The State of South Dakota made it an issue," Mr. Blouin said in an interview in
the teachers' lounge at Robert Lucas Elementary School after he had met the
sixth graders. He is one of four candidates seeking the Democratic nomination on
Tuesday to succeed Gov. Tom Vilsack, a Democrat who has decided not to seek
re-election after two terms.
A former congressman who in the 1970's pushed for a federal ban on abortion, Mr.
Blouin would have a simpler path if the questions went away. He said that he had
"transitioned on this issue" over the years — that although he remained "very
strongly anchored as a person who believes in life," he would oppose a ban if
one was passed by lawmakers. "I'd veto it in a heartbeat," he said.
One of Mr. Blouin's chief rivals, Chet Culver, the secretary of state, has made
his own support for abortion rights a central issue of his campaign, raising
doubts about Mr. Blouin's stance.
After shaking hands at the Hamburg Inn restaurant here this week, Mr. Culver
trumpeted his endorsement by Planned Parenthood of Greater Iowa's Political
Action Committee, the organization's first endorsement in a governor's race.
"A woman's right to choose is under assault, and people in this state are
absolutely worried," Mr. Culver said. "This has become a very important issue in
this state and in state races around the country — and it should be."
In Florida, the Democratic and Republican hopefuls for governor have staked out
sides over a state ban. On the Republican side, Charlie Crist has taken
criticism from some for seeming to shift on just how many exceptions he thinks a
ban should include — solely to save a woman's life or also when rape or incest
is involved.
In Arkansas, candidates in one Republican State Senate primary disagreed only
about when a state ban should come: before or after Roe v. Wade might be
overturned. In Ohio, both Republican hopefuls for governor — including J.
Kenneth Blackwell, the secretary of state and now the party's nominee — told
newspapers they would sign an abortion ban like South Dakota's if the State
Legislature were to pass such a bill.
In many state races, it remains uncertain who will benefit from the sudden focus
on abortion bans — candidates who oppose abortion rights or those who favor
them. Sometimes the political calculation gets complicated. While support for
bans has grown, especially in some Southern states, even those who oppose
abortion rights do not agree that direct challenges to Roe v. Wade are the best
approach. Some argue that gradual efforts to limit abortion are more likely to
win support.
"I think that, in the short term, this issue can be less helpful to pro-life
candidates," said Daniel McConchie, vice president of Americans United for Life,
a group that opposes abortion rights. "The questions that are being asked are
hypothetical, things governors mostly won't control. My concern is that the
average person on the ground will misinterpret the questions to be something
more real than they really are right now."
Jill June, president and chief executive of Planned Parenthood of Greater Iowa,
said that worry about the possibility of additional state bans was real and that
supporters of abortion rights had been stirred to action. "It now becomes much
more generally understood that a state really could outlaw it," Ms. June said.
"We know this is contagious, and we're fear-struck."
In South Dakota, Gov. Michael Rounds in March signed into law the nation's most
sweeping state abortion ban, a move intended to set up a direct court challenge
to Roe v. Wade. But opponents of the ban, which outlaws abortion except when the
mother's life is in jeopardy, have moved to challenge the law at the ballot box
instead. They filed petitions last month, hoping to send the question to voters
in November. On all sides of the issue, it is clear that some candidates might
have preferred for it not to grab quite so much notice.
Another Democratic hopeful for governor in Iowa, Ed Fallon, state representative
from Des Moines who has long supported abortion rights, said he would veto any
abortion ban.
But Mr. Fallon, who is viewed by some as the most liberal candidate (a label he
rejects), said he would rather spend his campaign talking about less
"politically polarizing issues," like campaign finance reform, health care,
education and the environment.
Sal Mohamed, a little-known candidate who is an engineer, said that he would
most likely veto a broad abortion ban, but he, too, suggested that the issue
might not warrant so much concern in the race here.
"I just don't think that we're going to get to that point in Iowa anyway," Mr.
Mohamed said.
But the terrain is most complicated for Mr. Blouin, who says he considers
himself "pro-life" but has, as he says, recognized that issues he considered
black and white in his 20's turned "fairly gray" later in life.
"Now you have a pro-life pro-choicer," said David Yepsen, the political
columnist for The Des Moines Register. "I don't think either side is happy with
him."
A Register poll, published in Sunday's editions, showed Mr. Culver winning among
36 percent of those surveyed, followed by Mr. Blouin with 28 percent, Mr. Fallon
with 21 percent and Mr. Mohamed with 1 percent. The survey of 600 likely voters
in the Democratic primary found 14 percent undecided. The poll had an error
margin of 4 percentage points.
Mr. Blouin, the state's former economic development director, has worked to hold
on to the support of those who may favor abortion rights. He picked as his
running mate Andrea McGuire, a physician who favors such rights.
But it is the abortion rights opponents who seem most irked at Mr. Blouin, once
a champion for their efforts. "He's a hypocrite," said Kim Lehman, executive
director of the Iowa Right to Life Committee. "He says he's pro-life, and yet
what he's really saying is that he is personally pro-life but would take no
action that's pro-life. He's the worst kind of so-called pro-life. I don't think
he has a right to call himself pro-life."
Whatever Democratic candidate emerges from the election on Tuesday (if none
garners 35 percent of the vote, the winner will be chosen at a state
convention), the questions about abortion are not going away; nor is the awkward
political terrain.
Representative Jim Nussle, Republican of Iowa, will face the Democratic nominee
in November. Asked repeatedly for an interview with Mr. Nussle about his views
on abortion, his spokeswoman, Maria A. Comella, said the candidate was too busy.
Ms. Comella provided Mr. Nussle's comments from a Radio Iowa interview on March
7, when he was asked about the possibility of an abortion ban here. "I'm 100
percent pro-life, and that's my voting record," he said, adding that he had
promoted a bill that would require parental consent for minors getting
abortions.
In the radio interview, Mr. Nussle said he did not believe the Iowa Legislature
would consider restrictions as "far reaching" as South Dakota's. He added, "I
will work with the Legislature if I have the opportunity to be governor to try
and ensure that parents have more of a direct impact on their kids' choices as
far as abortions are concerned."
But Mr. Nussle, his spokeswoman acknowledged, has yet to publicly answer this
season's question: to outlaw or not.
Gretchen Ruethling contributed reporting from Chicago for this article.
In State Races,
Tough Questions About Abortion, NYT, 5.6.2006,
http://www.nytimes.com/2006/06/05/us/05abortion.html
The State of AIDS,
25 Years After the First, Quiet
Mentions
June 5, 2006
By THE NEW YORK TIMES
On June 5, 1981, in the Morbidity and Mortality Weekly
Report from the federal Centers for Disease Control and Prevention, brief note
was taken of a peculiar cluster of pneumonia cases in five otherwise healthy gay
men.
The item was the first official mention of a scourge that had no name, no known
means of transmission, no treatment and no cure.
AIDS, as it would eventually be called, was already spreading fear in America's
gay enclaves, where before long half the young men who came of age at the dawn
of the gay liberation movement would be infected, stigmatized, ravaged by rare
infections and cancers, and die. It soon reached into neighborhoods already
burdened by poverty and drug abuse.
For years after that federal report, one of the few certainties was that this
disease, to quote other reports, was "invariably fatal." The United Nations
estimates that today, H.I.V., the virus that causes AIDS, has infected more than
65 million people, 25 million of whom have died.
Eventually, scientists discovered the virus that caused AIDS and a test to
screen for it. They learned the primary routes of transmission — unprotected
sexual intercourse, intravenous drug use and prenatal infection. They found a
cocktail of medications that slowed the disease's progression, at least in
America. In Africa and Asia, AIDS continues to cut a deadly swath.
The Nurse
The difference between then and now is stark for Joan Vileno, a nurse at
Montefiore Medical Center in New York. "In those days," she said, "all of our
patients died."
Ms. Vileno, 57, said she chose to start her career at an urban academic medical
center for the "unique experiences" that setting would provide. But she had no
idea how unique those experiences would be. "No textbook could prepare us for
what we were about to see," she said.
In the early 1980's, Ms. Vileno held the hands of angry, terrified and scorned
patients, mostly intravenous drug users. They were admitted with lethal
infections, rarely seen today, that left them gasping for breath, covered with
cancerous lesions, blind, demented and wasted to skin and bones.
There were no medications to cure them of a disease then called Gay Related
Immune Deficiency, or GRID, although at Montefiore, in the Bronx, the patients
were rarely gay. In a study of a drug that proved ineffective, the average
survival time of 300 Montefiore participants was eight months.
Today, Ms. Vileno runs a program for AIDS patients 50 and over who have lived
long enough to also have the medical problems that come with middle age.
But a quarter-century ago, absent any effective treatment, the staff improvised.
"The things we were able to do had nothing to do with our job descriptions," she
said.
Many patients were unwilling to come to the AIDS clinic lest they be seen by
someone they knew. So Ms. Vileno made house calls. Other patients, shunned by
family and friends, all but moved in to the ad hoc clinic — then a bit of
borrowed office space with a tiny staff; now a vast and humming operation.
Ms. Vileno once took a toddler home for the weekend so a husband could stay in
the hospital with his dying wife. She organized a wedding in the clinic,
officiated by a minister married to a staff member.
When funeral parlors refused to handle bodies, for fear of contagion, Ms. Vileno
found a willing undertaker and invited him to staff meetings so he would feel
like part of the team.
And returning from an AIDS conference in Paris, she went directly to the
hospital. Four patients had died that week, one of them estranged from his
family. He had designated Ms. Vileno his representative, so the morgue could not
release the body for burial without her signature.
"Everything we did was out of the box," she said. "People today think, 'What are
you talking about?' But it was a unique point in time, hopefully never to be
repeated."
JANE GROSS
The Mother
ATLANTA — Lisa Mysnyk describes the man who gave her H.I.V. as "one of those
African-American men who can't seem to stay out of jail." Still, she stayed with
him for three years. Sometimes they used condoms. Sometimes they did not.
Ms. Mysnyk, who is also black, now knows that "sometimes" can be a very
dangerous word.
"I got caught up in the idea that he wouldn't cheat on me," she said.
Just over half of new H.I.V. infections in the United States are in blacks,
according to the federal Centers for Disease Control and Prevention in Atlanta.
Three years ago, her boyfriend tested positive for the virus while in prison.
The staff made him call all his sexual partners to warn them about their own
risk. When he phoned Ms. Mysnyk, he said he had something to tell her, but he
could not seem to get it out. She finally heard the news from a prison nurse.
Her boyfriend called two other women that day, both of them younger than Ms.
Mysnyk, who was 34.
While she waited for her test results, Ms. Mysnyk, a single mother of two young
sons, told the doctor, "If I didn't have the Lord by my side, I'd be a nervous
wreck right now."
When the doctor told her she had H.I.V., Ms. Mysnyk started to cry. Her doctor
cried with her.
A few days later, she taught her younger son, who was 7 at the time, how to use
a condom. She had a no-nonsense conversation with her 14-year-old about sexually
transmitted diseases. "I didn't want him to ever have to be afraid," she said.
In the beginning, her own fear centered on how long she would live and what she
could do to keep herself alive. "I started taking all these medications," she
said, "and I never liked taking pills."
Ms. Mysnyk takes six pills a day, her virus level is undetectable and her immune
system continues to be strong. She thinks she could live 30 or 40 more years as
long as the drugs keep working.
She imagines that having the virus is a lot like having any other chronic
disease. But unlike most other diseases, she knows, H.I.V. can almost always be
avoided.
That is why, when she learned that a young woman who lives in her building was
coping with a second unplanned pregnancy, Ms. Mysnyk, rather than offering words
of sympathy, asked her a blunt personal question: "Do you and your boyfriend use
condoms?"
Her neighbor admitted that sometimes they did and sometimes they did not.
"Sometimes," Ms. Mysnyk told her, "isn't good enough."
BRENDA GOODMAN
The Prostitute
MUMBAI, India — With the strut of a baby-kissing politician, Mrs. Shah strolled
down the byways of the red-light district the other day, pausing every few steps
to offer a hug and a stern lecture to the prostitutes.
Mrs. Shah — tall and serene at 35, wearing a turquoise sari — began each
conversation gently, with a joke or a compliment. A woman's makeup, she might
say, was looking nice. Then she would lean in closer, glance around for
onlookers, and pull out a pamphlet from the AIDS organization for which she
works part time. Pointing at explicit photographs, she fired out her lessons:
This is how to wear a condom; this is what an infection looks like.
When her shift ends, Mrs. Shah, who is being identified only by her common last
name to help protect her identify, resumes her night job. By midnight, if luck
is kind, she will be in a cheap hotel, earning a few dollars from a strange man
for what she calls the only work she knows. And because she must survive, Mrs.
Shah will fail to tell him — even as she insists on a condom — that she is a
prostitute with H.I.V.
The United Nations reported recently that India had become the H.I.V./AIDS
capital of the world, its 5.7 million infections surpassing South Africa's 5.5
million. Some Indian officials have disputed that number, but the government has
acknowledged that the spread of the virus shows no signs of easing.
AIDS is often cast as an epidemic of bad choices. But it is also, in the life of
Mrs. Shah, an epidemic of the choiceless.
Since childhood, she has walked on a path leading, with ever greater inevitably,
to AIDS. At 13, she was forcibly married to a 35-year-old who kicked her out
when she complained of his infidelities. Days later, a woman found her on the
platform of a Bombay train station and offered to find her a job as a maid. By
evening, she had been sold to a brothel for 10,000 rupees, $220 today.
Once, she said, a customer became a lover, married her and took her away. When
he needed money, though, she was back on the street. She protested, and he
stabbed her in the cheek and back, burned her with kerosene on the belly and
legs and shaved her hip-length black hair down to the scalp.
Two years ago, a test found her H.I.V. positive. "I went crazy," she said. She
drank and took pills, trying to kill herself. Then social workers approached
her, looking for prostitutes to educate about AIDS.
"I had an idea," she said over a cup of tea, "that what happened to me, I would
not let happen to other girls."
ANAND GIRIDHARADAS
The Researcher
SAN FRANCISCO — Work on AIDS remains his calling, but the grand emotions of the
early years have subsided. Today, both the disease and Dr. Paul A. Volberding, a
physician and researcher who is graying and has an arthritic curl to his
fingers, have settled in.
Strangers on airplanes no longer accost him with questions about quick cures,
and young men no longer die in his arms. Now if a patient dies, he said, "We
think we've done something wrong."
Dr. Volberding, 56, who for many years ran the AIDS program at San Francisco
General Hospital, now heads medical services at the San Francisco Veterans
Affairs Medical Center. These days his AIDS research, like much of the pandemic,
is focused on Africa.
"It feels good to do something so clearly needed that improves health so
dramatically," he said of his work in Uganda.
Dr. Volberding has been touched by AIDS since July 1, 1981, his first day at San
Francisco General, when he treated a 22-year-old gay man with Kaposi's sarcoma,
a disease that until then was seen mostly in the elderly. After he came across
other cases, Dr. Volberding did what academics often do: He studied them.
Because established physicians lacked the time and often the inclination to take
on what was known as the gay disease, the field was wide open. At 31 and with a
staff of one (himself), Dr. Volberding opened one of the first clinics anywhere
for people with the disease. A year later, with assistance, he began conducting
small clinical trials.
"The patients were so much like us," Dr. Volberding said. "We were all young."
Many of them, he recalled, listened to the same music. He still keeps an old
Grateful Dead poster on his office wall.
In those early years, Dr. Volberding and his colleague, Dr. Marcus Conant, both
professors at the University of California at San Francisco School of Medicine,
listed every patient in the city on a blackboard. They knew each by name.
Financing was scarce. Dr. Volberding remembered Dr. Conant suggesting that they
wait until there were 1,000 cases, and then the government would take notice.
Many researchers thought they, too, were at risk. Both Dr. Volberding and his
wife, Dr. Molly Cooke, also a physician, experienced such fears. Once when Dr.
Volberding found a blotch on his skin, colleagues had to reassure him it was not
Kaposi's sarcoma. All that has changed, too. Today, Dr. Volberding said, he and
his patients commiserate mostly about arthritis and aging.
CAROL POGASH
The Artist
Art is forced by crisis to become political, and so it has been with AIDS, says
the playwright Tony Kushner. The early works came in partly as a response to a
society that was slow, even resistant, to accept the reality of a new pandemic.
"It was so clearly the dominant culture's mandate that AIDS death and AIDS
suffering should be silenced," Mr. Kushner said. "The obvious thing to fight it
would be to speak of it and articulate it."
What followed were works like Larry Kramer's 1985 play, "The Normal Heart," and
Mr. Kushner's own Pulitzer Prize-winning 1993 drama, "Angels in America."
Only recently, he said, did he begin to reflect on the impact that the early
years of AIDS had on the creative culture, especially on writers and artists.
"We were a community that was in a certain sense ideal in terms of responding in
an organized fashion," Mr. Kushner said. "As soon as it became an issue of
poverty, it lost a degree of organizational support, as soon as it became more
or less brought under control in certain ways in the U.S.," he said. "You can't
sustain rage for decades."
The great hole in the landscape is hard to comprehend even now, years past the
time when AIDS was ravaging the American art world unchecked.
"There's a group of gay men about five years older than me who no longer exist,
who would still be alive and producing work, who are gone," said Mr. Kushner,
49. "And there are a number of people I know who survived the epidemic but who
in a certain sense didn't survive, who entered a permanent state of mourning."
CAMPBELL ROBERTSON
The Pioneer
Twenty-five years ago, Lawrence D. Mass was running an addiction treatment
program in Manhattan for Greenwich House, a social services group whose clients
included drug abusers and gay men.
Fertile ground, it turned out, for first documenting the disease that would
become known as AIDS.
A little-known physician, Dr. Mass wrote what AIDS chroniclers regard as the
first article on the emergence of — well, of something unusual and terrible, but
exactly what was not clear at the time. The article appeared in The New York
Native, a small weekly written for a gay audience, on May 18, 1981, several
weeks before the first scholarly journal weighed in.
Dr. Mass, who is gay, went on to become a founder of Gay Men's Health Crisis and
to devote much of his life to fighting the disease he had stumbled onto.
In early 1981, Dr. Mass, then 34, had heard fragments of rumors about strange
health problems cropping up in Lower Manhattan, especially among gay men. He
found Dr. Steve Phillips, an epidemiologist with the Centers for Disease Control
and Prevention, who was following the new mystery. Based on his conversation
with Dr. Phillips, Dr. Mass wrote a short article about "rumors that an exotic
new disease had hit the gay community."
There was so little anyone knew at first, and so much that people got wrong. But
looking back, said Dr. Mass, who still practices medicine in Manhattan, there is
one essential truth he believes he had right all along.
"From the start, I said you need to acknowledge our civil rights, you need to
recognize our relationships, to have any chance of containing and preventing
AIDS," he said. "Shame and fear make it worse."
RICHARD PÉREZ-PEÑA
The Friends
PROVINCETOWN, Mass. — Jay Critchley's recollection of what happened when AIDS
first hit this gay-friendly town on the tip of Cape Cod is clear and stark.
"People just disappeared and died," he said. "It was that dramatic, and it was
frightening."
It was common to see men with lesions walking in and out of the shops,
bookstores and restaurants that line the town's main street, struggling to
breathe the salt air, said Mr. Critchley, an artist and massage therapist.
Asking someone if he had lost weight was taboo; it meant asking if he was sick.
Friends made sure to stay in close contact, because those who fell out of touch
were usually dying.
The town's gay residents drew together and cared for the sick. Many went house
to house, making sure they were comfortable, safe, well fed. Still, no one
understood the provenance of the suffering, and when investigators from the
federal Centers for Disease Control and Prevention came to town on a
fact-finding mission, many gay men simply assumed that they, too, would get sick
and die quickly.
"There was a time when I just waited for it to happen to me," said Tom Sterns,
an antique shop owner and 30-year resident. "There wasn't any point in getting
tested because they couldn't do anything for you, and I didn't want to face
having it."
In the mid-1980's, he finally got tested. The results were negative.
AIDS changed Provincetown itself, for good and bad. In the summer of 1983, many
tourists stayed away, fearful of contracting the disease. But gay men in the
once carefree community grew cautious about unsafe sex, Mr. Critchley said.
As advances in drug treatment have allowed infected men to lead longer,
productive lives, the disease is no longer visible, Mr. Sterns said, and is not
in the forefront of every gay man's mind.
But that is leading to more problems, said Mr. Critchley, who sees more men
slipping back into careless sexual practices.
With the reduction in fear, the town too has changed. Rising real estate prices
and an influx of tourists have chipped away its neighborliness and bohemian
flair.
"The town is so dramatically different now than it was 10 years ago," Mr.
Critchley said.
KATIE ZEZIMA
The State of AIDS,
25 Years After the First, Quiet Mentions, NYT, 5.6.2006,
http://www.nytimes.com/2006/06/05/health/05aids.html
Profile: Generation AIDS
Updated 6/4/2006 11:03 PM ET
USA Today
By Steve Sternberg
Twanashia Clark grew up in sweltering Houston streets
teeming, she says, with "guns, gangs and drugs," where poverty and despair
masked a more sinister threat: HIV, the AIDS virus.
Few people, if any, suspected that HIV might someday pose a
threat to young people like Clark when federal health officials warned on June
5, 1981, that five homosexual men in Los Angeles had fallen prey to a rare form
of pneumonia.
Today, on the 25th anniversary of that report, 65 million people are infected
with HIV worldwide and more than 25 million have died, reports the Joint United
Nations Programme on HIV/AIDS (UNAIDS). Clark, 24, belongs to the first
generation of young adults, ages 18 to 25, who have never known a world without
AIDS.
She says her diagnosis, on Oct. 10, 2000, influenced every aspect of her life,
even prompting her to give her children, Daelon, 5, and Daejhanie, 10 months,
similar names. "I want them to know that they are born of each other," she says,
"and when they grow up, they're still going to need each other, in case I'm not
around to remind them."
Clark represents how much has changed since the early days of the epidemic.
Today, about one-third of new infections are transmitted heterosexually, up from
3% in 1985, reports the Centers for Disease Control and Prevention. More than
half of those diagnosed with HIV are black, up from 25% in 1986, though blacks
account for about 12% of the population. Black women and black gay men are
especially at risk.
Infection rates among black women in the USA are 20 times higher than for white
women and five times higher than among Hispanic women. Two-thirds of HIV
infections in young women like Clark result from unsafe sex with infected
partners, the CDC says. "More than half the women we treat had one sexual
partner and no idea he was HIV-positive," says Donna Futterman, director of
adolescent AIDS at Montefiore Medical Center in New York.
A CDC study of 1,767 gay men in five U.S. cities found that almost half of all
blacks were infected and many didn't know it.
Rudolph Carn, 50, of Atlanta, a founder of the National Black Gay Men's Advocacy
Coalition, says the high rates should come as no surprise in a community where
homophobia is widely accepted, AIDS carries a weighty stigma and gay children
are sometimes treated as outcasts. "The parents actually think they're morally
right," Carn says. "They feel compelled to throw them out."
AIDS' stigma is nothing new. When news of the epidemic broke in 1981, tabloids
quickly labeled it the "gay plague." Even some doctors began calling it "GRID,"
for "gay-related immune deficiency."
Doctors would soon learn that AIDS comes in many guises. Within months,
researchers would report that the disease had turned up in infants, Haitians,
needle-sharing drug abusers, transfusion recipients and hemophiliacs, including
a Hollywood, Fla., man in his 70s who gave the disease to his wife of 50 years.
The couple, diagnosed in 1983, made it clear that AIDS could spread
heterosexually as well.
The lingering impression that AIDS is a gay disease helped promote its spread
among blacks, says Pernessa Seele, founder of Balm in Gilead, a New York-based
AIDS advocacy organization that works with 15,000 churches nationwide.
"The fundamental problem with the African-American community is that information
about HIV came at us wrong," she says. "It came to us that this was a gay white
disease, you don't have to worry about it. Then it was homosexuals and drug
addicts. We're still suffering from the wrong information."
Many young people harbor misconceptions about HIV, according to a 2006 survey of
18- to 25-year-olds by the Kaiser Family Foundation. Nearly 60% don't realize
that having another sexually transmitted disease increases their HIV risk; 30%
don't realize you can't get AIDS from kissing. Although the survey's margin of
error is plus or minus 7 percentage points, the findings are consistent with an
overall survey of 2,517 respondents of all ages, with a margin of error of plus
or minus 2 percentage points.
HIV exploits misinformation, relaxed sexual attitudes, poverty, drug abuse,
prostitution and denial of personal risk. The virus also benefits from
globalization, as millions of people crowd into cities and travel worldwide,
multiplying opportunities for sexual encounters that spread the disease.
It's a stealth virus, too
The virus's long incubation period also works in its favor. Because they might
not feel sick for years, many people don't realize they're HIV-positive until
they've infected others, says James Curren, dean of public health at Emory
University, who led the CDC's first AIDS task force. "Problems like SARS and
bird flu come fast and leave fast. HIV comes slowly. It's creeping up as a cause
of death and won't stop."
When AIDS emerged, Curran says, some doctors believed viruses would never
surrender to treatment. A drug discovery effort, driven partly by an explosion
of deaths and activism by white gay men, proved them wrong.
Taking the lead was a New York-based group called ACT UP, founded in 1987 with
the credo: Silence Equals Death. ACT UP activists chained themselves to drug
company headquarters and shouted down speech-making politicians to draw
attention to the epidemic.
"The scary thing," says activist Eric Sawyer, 53, "is that when we founded ACT
UP during the Reagan administration, the number of reported cases of AIDS were
in the tens of thousands. If people had just listened to the (gay) community, we
wouldn't have 65 million infections and 20 million deaths."
The first AIDS drug, zidovudine, won federal approval in 1987. A decade later,
scientists reported that highly active retroviral drug cocktails, known as
HAART, could virtually eliminate the virus from the blood, turning AIDS into a
chronic, manageable disease.
But understanding how to treat HIV is one thing; figuring out how to stop the
epidemic is another. A two-decade effort to develop an effective vaccine has
been fruitless.
Conflicting attitudes about sex education, condom use and morality hinder
prevention efforts, says Myisha Patterson, 27, a health specialist for the
Baltimore-based National Association for the Advancement of Colored People.
"I don't remember hearing about HIV until middle school, when we had family-life
education classes," she says. "At that time, AIDS was still considered a disease
of gay white men. It was for me until I went to college and focused on health
care."
Family-life classes have become a flashpoint in the debate about HIV prevention.
In 2006, the Bush administration requested $206 million, up from $168 million in
2005, to fund educational programs that promote sexual abstinence before
marriage and highlight the shortcomings of safer sex practices, including condom
use.
"It's all because people don't want to accept that people, especially young
people, have sex," Sawyer says. "To not arm young people to have sex
responsibly, in a way that will protect their lives, is unconscionable."
The CDC's Ronald Valdeserri says: "CDC's official policy is to say that
abstinence is the most effective way of preventing HIV and other STDs, but we
recognize that there are some young people who are sexually active. For those
young people, we have messages like have a single partner, try to know (whether
he or she is infected). If you don't know, consistent and correct use of a
condom can lower your risk."
'I didn't know he was infected'
Clark, now an AIDS activist and educator, says she had so much to deal with as a
child that her HIV risk never entered her mind. "My mother was a diabetic, and
she was sick," she says. At 14, she was giving her mother insulin shots. Her
father, a drug dealer, was in and out of prison. Both died while Clark was still
in her teens.
Her aunt decided to pull Clark from school and teach her at home after she
passed out during classes from insulin shock, an indication that she had
inherited her mother's diabetes. She was 16.
No parents and no school meant no sex education, though she had become sexually
active. "It was scary; I knew that I was on a road I didn't want to be on," she
says. "By 17, I was in a steady relationship with a man who was infected. I
didn't know he was infected."
Clark's diagnosis came during a routine prenatal exam while she was pregnant
with her son, Daelon, born Dec. 1, 2000. Her biggest worry wasn't her health,
but his. Both of her children have been spared AIDS by one of the biggest AIDS
breakthroughs, a short course of therapy that has dropped the number of
HIV-positive newborns from 1,800 a year in the early '90s to fewer than 100
today.
Spreading the word
Monica Johnson, 22, Sandra Jeter and Janeé Herndon, both 15, are unwilling to
leave the AIDS fight to their elders. Members of a group called the Young Women
of Color Leadership Council, sponsored by the non-profit Metro TeenAIDS in
Washington, D.C., they counsel classmates, hand out condoms and staff tables at
public gatherings to get the word out about AIDS.
Few young Americans face a challenge more daunting than trying to turn the tide
on AIDS in a city where roughly one of every 20 residents is HIV-positive, and
where the AIDS rate of 179 per 100,000 is roughly four times that of any state.
Sprawled on couches recently amid festive homemade HIV prevention posters in
Metro TeenAIDS headquarters not far from the U.S. Capitol, they discussed coming
of age in the AIDS generation.
"Everybody I associate with, they're having sex," says Janeé, who attends
Spingarn Senior High. "Some little girls think it's cool to have sex."
Despite the long odds, these young women aren't giving up. Johnson, a high
school graduate who works part time at MetroTeen AIDS, says that when someone
tells her "I don't want to talk," she responds, "Two minutes could save your
life."
Profile:
Generation AIDS, UT, 4.6.2006,
http://www.usatoday.com/news/health/2006-06-04-aids-anniversary_x.htm
No Compromise in Sight on Plan to Fight H.I.V.
June 4, 2006
The New York Times
By DAVID W. CHEN
TRENTON, May 31 — In every legislative session here but one
since 1992, at least one bill has been introduced to allow drug users to
exchange used syringes for new ones. And though the details have differed from
year to year, one goal has remained constant: to reduce the spread of H.I.V. in
a state with one of the nation's highest infection rates.
But 14 years later, New Jersey remains one of only two states — the other is
Delaware — that still prohibit both needle exchanges and access to syringes at
pharmacies without a prescription.
No one disputes that H.I.V. and AIDS are major public health problems in New
Jersey. The state has the country's highest rate of H.I.V. infection among
women, who make up 36 percent of the cases among New Jerseyans over 13, and the
third highest among children. Over all, almost 33,000 people in New Jersey have
AIDS, up from 26,000 at the end of 1998. Forty-one percent of all cases resulted
from injection drug use, according to the state health department.
Yet in New Jersey, the effort to make needles freely or more easily available
has been blocked repeatedly over the years. Gov. Christie Whitman, a Republican,
adamantly opposed the idea, for instance, while Gov. James E. McGreevey, a
Democrat, dropped his support in the face of opposition from police chiefs and
some legislators.
Now Gov. Jon S. Corzine and the State Assembly are determined to legalize needle
exchanges. But once again, the effort is being blocked, this time in the State
Senate, where Ronald L. Rice, a Democrat, has struck an alliance with Republican
lawmakers, who are in the minority, to keep the legislation bottled up in
committee.
To Mr. Rice and other critics, including John P. Walters, the director of the
White House Office of National Drug Control Policy, making needles more
accessible suggests that government is condoning an illegal — and destructive —
activity. They favor educational campaigns and treatment programs to discourage
drug use.
"Needle exchange is a form of keeping people junkies the rest of their lives,"
said Mr. Rice, a former Newark police officer.
"You don't wipe out a whole lot of people by gassing them," he said. "And you
don't wipe people out like the Tuskegee Institute, where we had a bad
experience.
"That's what you're doing with this needle exchange," Mr. Rice said. "Those
aren't offensive statements; those are examples of what people have been doing
to people, and it shouldn't be."
Supporters of needle exchanges counter that they are backed by just about every
major scientific or medical organization, including the National Institutes of
Health, the American Medical Association, the Centers for Disease Control and
Prevention and, closer to home, the New Jersey Hospital Association.
In New York City, studies have shown that such programs had reduced the rate of
new H.I.V. infections by roughly 75 percent since the 1990's, according to Dr.
Don C. Des Jarlais, the director of research for the Baron Edmond de Rothschild
Chemical Dependency Institute at Beth Israel Medical Center.
He cautioned that individual studies might have had flaws, but emphasized that
"the sum of these less-than-perfect studies is sufficiently conclusive: All of
the research syntheses have come to the conclusion that the programs can and do
work."
Across the Hudson, meanwhile, Governor Corzine has said that one of his biggest
disappointments since his inauguration in January has been the lack of progress
toward a needle exchange program.
Other officials have voiced similar complaints.
"It's a disgrace, a disgrace, that we are so far out of step with other states,"
said Assembly Speaker Joseph J. Roberts Jr., a Democrat from Camden County.
Noting that California recently made it easier to buy syringes without
prescriptions, Mr. Roberts added: "That great liberal voice Arnold
Schwarzenegger has been able to tackle this issue, but New Jersey hasn't. We've
allowed a few people who have had very loud voices to demagogue the issue and to
tie it up, and people are dying each and every day."
The late Senator Wynona M. Lipman, a Democrat, introduced the first
needle-exchange bill in 1993. Republicans controlled the Legislature for most of
the 1990's, though, and Governor Whitman was one of the most vocal opponents.
In 1996, Mrs. Whitman appointed David W. Troast, a wealthy businessman and
social acquaintance from Somerset County, as the head of the state's Advisory
Commission on AIDS. But much to everyone's surprise, he endorsed needle exchange
after interviewing experts in public health, AIDS prevention and epidemiology.
"There is nothing that we can come up with as effective as a clean-needle
program and the retail distribution of needles," Mr. Troast said at the time, a
stance that prompted a public spat with Mrs. Whitman.
By the time the Democrats regained control of the Legislature in 2002,
needle-exchange supporters were more optimistic. But it was not until after Mr.
McGreevey announced plans to resign in August 2004 that he got behind the effort
and issued an executive order authorizing pilot exchange programs in Camden and
Atlantic City.
Mr. Rice and three Republican legislators, including State Senator Thomas H.
Kean Jr., who is now running for the United States Senate, quickly went to court
and blocked those programs.
"If the governor could go so greatly beyond his executive order to obviate
criminal standards, that was a very bad precedent," Mr. Kean said. "It sends the
absolute wrong message to the youth of our state."
Mr. Rice has often worked with Republicans on the Senate health committee, like
Mr. Kean, to prevent his Democratic colleagues from garnering a majority of
votes. There are five Democrats and three Republicans now, so Mr. Rice's
opposition virtually guarantees a deadlock.
Senate Democrats tried earlier this year to expand the health committee by
adding Senator Loretta Weinberg, a Bergen County Democrat and needle-exchange
advocate, but the proposal fizzled out. Some legislators and aides have said
that Democrats were uncomfortable expanding a committee just to push through one
bill.
One ardent needle-exchange supporter, Senator Nia H. Gill, a Democrat, has vowed
to use her privilege of "senatorial courtesy" to block nominees to various
governmental entities when they are from her home county, Essex, and are
supported by the Senate president, Richard J. Codey, also from Essex.
She wants him to use his power to bring the needle measure directly to the
Senate floor for a vote, bypassing Senator Rice and his Republican allies. But
Mr. Codey, a supporter of needle exchange, has been loath to do so, in part
because it would break Senate protocol.
"It's about invoking your power and using it for people who have little or no
voice in the process," Ms. Gill said.
In another maneuver, some legislators and aides say Mr. Roberts, the Assembly
speaker, may be holding up passage of one of Mr. Codey's signature causes, a
stem cell research bill, until needle-exchange legislation passes. When asked
about a possible link, Mr. Roberts demurred and said only that "we're going to
get this done, and I need some help in the Senate to get it done."
But he also said that he was "hopeful they'll both be advanced before we leave
in June."
In recent weeks, Mr. Corzine has also made more noise, prompting speculation
that he, Mr. Codey or Mr. Roberts might try to find a creative compromise soon.
"He has signaled a more aggressive stance and a willingness to speak out," said
Anthony Coley, Mr. Corzine's press secretary. "We have an opportunity here to
save people's lives, and that's not overstating the case."
Mr. Rice says he is frustrated that his $100 million proposal for residential
substance abuse treatment centers has gotten no traction, while proposals on
mental health and stem cell research totaling more than $400 million have either
become, or are close to becoming, a reality. Yet he says he also knows that his
longtime efforts may come up short.
"I may lose the battle at the end, but I'm never going to vote — never," said
Mr. Rice, who recently lost the Newark mayor's race. "I'll die before I give a
vote to give free needles to people."
Richard G. Jones contributed reporting to this article
No Compromise in
Sight on Plan to Fight H.I.V., NYT, 4.6.2006,
http://www.nytimes.com/2006/06/04/nyregion/04needles.html
A Spoonful of Foreign Culture
Helps Western Medicine Go
Down
June 4, 2006
The New York Times
By NICHOLAS CONFESSORE
When officials at Brooklyn's Maimonides Medical Center were
preparing a new clinic in Sunset Park in April, everything was ready for the big
opening day except the big opening day itself.
"One of our staff members told us it was an unlucky date," said Pamela S. Brier,
the hospital's chief executive. "We had to change it."
So the ribbon-cutting, originally scheduled for April 24, was moved to the
following day. It was a difference of only 24 hours, but all the difference in
the world to the Chinese immigrants the clinic was largely built to serve, who
believed the 25th to be a more auspicious date.
It was one of the many ways in which the $1 million clinic was carefully
designed to cater to Sunset Park's fast-growing Chinese population, one of the
largest in the city.
Because the color white is associated with death in China, the walls are mostly
painted in yellow and pink tones. And because Chinese immigrants have high rates
of tuberculosis infection, every patient is tested for it. The chefs in the main
hospital's kosher kitchen have learned to prepare rice porridge, a beloved
Chinese comfort food. "Language, culture, food — it's all tremendously
important," Ms. Brier said.
The new clinic is Maimonides's most ambitious effort to respond to a growing and
increasingly diverse population of immigrant patients. It also reflects a
broader national shift in health care as urban hospitals move beyond the
translation services that started becoming common in the late 1990's and
acknowledge that language is not the only barrier they face in treating people
from all over the globe.
Some come from cultures that are broadly skeptical of Western medicine, and
prefer the herbs and poultices of traditional healers, "cures" that in some
cases can retard the effects of prescribed medicines or produce dangerous
interactions. Others come from cultures where they are expected to hide sickness
from strangers, or where it might be offensive for male doctors to examine
female patients.
"It's been a slow trend to develop because it's not always clear to a hospital
how big a certain community might be, and sometimes it takes a couple of years
to manifest," said Rick Wade, a senior vice president of the American Hospital
Association. But now, he said, programs are appearing everywhere, to strengthen
what hospitals call "cultural competency."
At Oakwood Hospital in heavily Arab Dearborn, Mich., nurses are trained to point
the beds of Muslim patients toward Mecca. In Glendale, Calif., which had a rapid
influx of Armenian immigrants during the 1990's, one hospital sponsors a popular
health-related call-in show that is broadcast in Armenian on cable-access
television.
But challenges can be more varied and daunting for hospitals in places like
Brooklyn, home to insular communities of Orthodox Jews, Muslims from
conservative Arab countries, recent immigrants from rural China and Hispanics
from Central and South America, among many others.
"In each culture that we're dealing with, there are different ideas, family
values and beliefs, whether about medicine or life in general," said Virginia
Tong, a vice president at Lutheran Medical Center, one of south Brooklyn's
largest health care providers. "Let's say you had an Hispanic godparent who
brought a patient in to see a doctor. In this country, we would say, 'That's not
a parent;' there might be legal issues. But in their culture, godparents are
almost as important as parents."
Lutheran's main hospital has a mosque on site; it also runs clinics aimed at
Caribbean and Korean immigrants. In 2001, Lutheran opened its own Chinese
clinic, on Eighth Avenue in Sunset Park, after a survey showed that most Chinese
immigrants in the area were going to Chinatown in Manhattan for medical care.
Maimonides, long known as "the Jewish hospital," in Ms. Brier's words, has in
recent years customized the care at many of its 15 clinics, which are around
southwest Brooklyn, based on the cultures and needs of the patients each serves.
The doctors at the hospital's Newkirk Avenue clinic, for example, see many
Indian immigrants, who have disproportionately high rates of hypertension. Its
pediatricians also see many children born in Bangladesh. Because infants there
are often not immunized against measles, as most babies are in the United
States, that means more effort devoted to vaccination and extra care in
reporting cases to public health officials to contain any outbreaks.
But the hospital's outreach to Chinese immigrants is its biggest, driven by what
its officials believe will be continued population growth in south Brooklyn. "We
go where the patients are," Ms. Brier said.
Maimonides opened its first Sunset Park clinic in a brownstone building in 1996.
Within three years, doctors there were seeing 9,000 patients a year, including a
growing number of Chinese. The number of patients has doubled since, prompting
the latest move from a storefront space to a 10,000-square-foot building on
Seventh Avenue and 64th Street.
The attending doctors there speak Mandarin or Cantonese, two major Chinese
dialects. About 70 percent of the patients are Chinese, according to Dr. Bing
Lu, the clinic's medical director, and a significant number are recent arrivals
to the United States. Many hold the traditional belief, he said, that drawing
blood for tests drains a person's life force, and they are reluctant to allow
it.
"We teach them that they need it," he added, relying on the staff members'
language skills and familiarity with Chinese culture to reduce patients'
suspicion. "Generally speaking, Chinese people don't believe in preventative
care."
Such an attitude can be deadly. A few years ago, doctors at the clinic found
early signs of liver cancer in a man in his 30's who was infected with hepatitis
B. The man left the clinic, Dr. Lu said, and did not return the clinic's phone
calls. When he finally came back six months later, he was jaundiced and
underweight, with a severely enlarged liver. The cancer had advanced beyond the
possibility of life-prolonging surgery.
It was "a fatal mistake," said Dr. Lu, who believes the man at first sought out
traditional healers instead of returning to the clinic.
Several patients praised the doctors' warmth and staff members' willingness to
help them with paperwork. Susan Lin, 31, who emigrated from China's Fujian
Province five years ago, said, through an interpreter: "Sometimes we're afraid
to ask questions, to ask how to follow up. Here, they always smile, they are
always welcoming. You feel very comfortable asking questions."
Recently, an 80-year-old woman arrived at the clinic just before closing time,
asking to see a doctor. She said it was urgent, but when examined she would say
only that she had been unable to sleep for about a week.
Under careful questioning, Dr. Lu said, she eventually revealed that her husband
had died the previous week, and that she had been crying and having anxiety
attacks, details that a Chinese woman her age might consider inappropriate to
admit.
"When you know the culture, you know it's normal, but if you don't, as a
practitioner, you can miss a significant problem," Dr. Lu said. "She could
easily have been turned away from the clinic that day."
A Spoonful of
Foreign Culture Helps Western Medicine Go Down, NYT, 4.6.2006,
http://www.nytimes.com/2006/06/04/nyregion/04clinic.html
Louisiana House OK's Ban on Most Abortions
June 1, 2006
By THE ASSOCIATED PRESS
Filed at 12:35 a.m. ET
The New York Times
BATON ROUGE, La. (AP) -- The Louisiana House approved a ban
on most abortions, a largely symbolic bill that could go into effect only if the
U.S. Supreme Court's landmark 1973 decision is overturned.
The measure would allow abortion in cases when the woman's life is in danger or
childbirth would permanently harm her health. The bill passed 85-17 and heads to
the Senate.
It could take effect only under two circumstances: if the U.S. Constitution is
amended to allow states to ban abortion; or if the U.S. Supreme Court strikes
down its own Roe v. Wade ruling, which provided for a woman's right to an
abortion.
The bill is similar to a South Dakota law passed this year that is expected to
land before the high court.
Passage of the Louisiana bill was not in doubt; the fight centered on whether to
allow exceptions for rape and incest victims. The amendment failed after
opponents argued that the bill should prevent as many abortions as possible.
Under the bill, doctors found guilty of performing abortions would face up to 10
years in prison and fines of $100,000.
Gov. Kathleen Blanco, who campaigned as an anti-abortion candidate, has not said
whether she would support such a strict ban.
Louisiana House
OK's Ban on Most Abortions, NYT, 1.6.2006,
http://www.nytimes.com/aponline/us/AP-Abortion-Ban.html
|