|
History > 2011 > USA > Health (I)
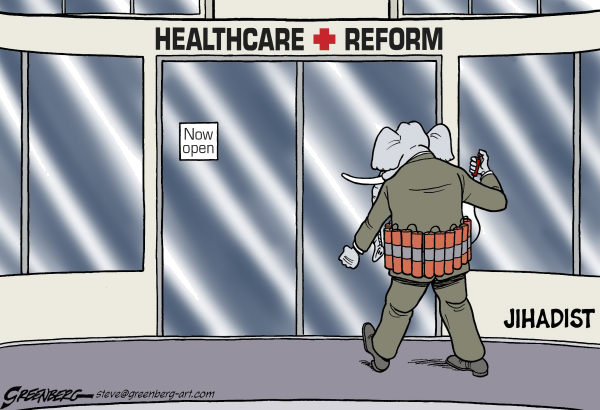
Steve Greenberg
The Ventura County Star
CA
Cagle
6 January 2011
Elephant = Republicans
20% Rise Seen
in Number of Survivors of Cancer
March 10, 2011
The New York Times
By PAM BELLUCK
About one in every 20 adults in the United States has survived cancer,
including nearly one-fifth of all people over 65, according to new federal data.
The numbers, released Thursday by the Centers for Disease Control and Prevention
and the National Cancer Institute, indicated that the number of cancer survivors
increased by about 20 percent in just six years, to 11.7 million in 2007, the
latest year for which figures were analyzed, from 9.8 million in 2001. In 1971,
the number of cancer survivors was three million.
“There’s still a concept that cancer is a death sentence,” said Dr. Thomas R.
Frieden, director of the Centers for Disease Control. But, he said, “for many
people with cancer there’s a need for them and their families and caregivers to
recognize that this is a stage. They can live a long and healthy life.”
About 65 percent of cancer survivors have lived at least five years since
receiving their diagnosis, 40 percent have lived 10 years or more, and nearly 10
percent have lived 25 years or longer.
The implications, Dr. Frieden said, are that many cancers are treatable and that
it is just as important for people who have had cancer not to assume that they
will necessarily die early.
“You might think, ‘I’ve had cancer — I don’t have to worry about eating right,
quitting smoking, exercising,’ ” Dr. Frieden said. But people with cancer “need
to be just as concerned about heart disease and other risks as they would
otherwise,” he said.
The study defined a survivor as anyone who ever received a diagnosis of cancer
who was alive on Jan. 1, 2007, and it did not indicate if the person was cured,
undergoing treatment, afflicted with a chronic cancer-related illness, or in the
process of dying at that time.
And the numbers tell only a piece of the cancer story. Some cancers, like lung
cancer, are aggressive and difficult to treat. And the death rate from cancer,
an indicator that many health experts consider a more accurate measure of
progress in fighting the disease, has stayed virtually the same as it was in
1950 — about 200 deaths per 100,000 people a year, and about 1,000 deaths
annually per 100,000 people over 65.
Dr. Frieden said the increase in cancer survivors was due to several factors,
some of which varied by type of cancer. In some cases of breast cancer and colon
cancer, for example, improved treatment and increased follow-up after treatment
have helped increase survival. In others, like prostate cancer, an explosion in
screening has identified many men with the disease, but the cancer is often so
slow-growing that they would be unlikely to die from it. And other cancer
diagnoses are simply the consequence of the country’s aging population and
improved care for other diseases — in other words, people are living long enough
to develop cancer.
About a million more of the survivors were women than men, partly because women
live longer than men, and partly because breast and cervical cancers are often
diagnosed and treated at younger ages. About 22 percent of the survivors had
breast cancer, about 19 percent had prostate cancer, and about 10 percent had
colorectal cancer.
The study identified only the type of cancer first diagnosed in each person;
additional tumors or cancer diagnoses were not recorded.
Health authorities urged families and physicians to be aware of the health needs
of cancer survivors.
“Having cancer may be the first stage, really, in the rest of your life,” Dr.
Frieden said. “We need to continue to scale up” the services available for
cancer survivors.
20% Rise Seen in Number
of Survivors of Cancer, NYT, 10.3.2011,
http://www.nytimes.com/2011/03/11/health/11cancer.html
Talk Doesn’t Pay, So Psychiatry Turns to Drug Therapy
March 5, 2011
The New York Times
By GARDINER HARRIS
DOYLESTOWN, Pa. — Alone with his psychiatrist, the patient confided that his
newborn had serious health problems, his distraught wife was screaming at him
and he had started drinking again. With his life and second marriage falling
apart, the man said he needed help.
But the psychiatrist, Dr. Donald Levin, stopped him and said: “Hold it. I’m not
your therapist. I could adjust your medications, but I don’t think that’s
appropriate.”
Like many of the nation’s 48,000 psychiatrists, Dr. Levin, in large part because
of changes in how much insurance will pay, no longer provides talk therapy, the
form of psychiatry popularized by Sigmund Freud that dominated the profession
for decades. Instead, he prescribes medication, usually after a brief
consultation with each patient. So Dr. Levin sent the man away with a referral
to a less costly therapist and a personal crisis unexplored and unresolved.
Medicine is rapidly changing in the United States from a cottage industry to one
dominated by large hospital groups and corporations, but the new efficiencies
can be accompanied by a telling loss of intimacy between doctors and patients.
And no specialty has suffered this loss more profoundly than psychiatry.
Trained as a traditional psychiatrist at Michael Reese Hospital, a sprawling
Chicago medical center that has since closed, Dr. Levin, 68, first established a
private practice in 1972, when talk therapy was in its heyday.
Then, like many psychiatrists, he treated 50 to 60 patients in once- or
twice-weekly talk-therapy sessions of 45 minutes each. Now, like many of his
peers, he treats 1,200 people in mostly 15-minute visits for prescription
adjustments that are sometimes months apart. Then, he knew his patients’ inner
lives better than he knew his wife’s; now, he often cannot remember their names.
Then, his goal was to help his patients become happy and fulfilled; now, it is
just to keep them functional.
Dr. Levin has found the transition difficult. He now resists helping patients to
manage their lives better. “I had to train myself not to get too interested in
their problems,” he said, “and not to get sidetracked trying to be a
semi-therapist.”
Brief consultations have become common in psychiatry, said Dr. Steven S.
Sharfstein, a former president of the American Psychiatric Association and the
president and chief executive of Sheppard Pratt Health System, Maryland’s
largest behavioral health system.
“It’s a practice that’s very reminiscent of primary care,” Dr. Sharfstein said.
“They check up on people; they pull out the prescription pad; they order tests.”
With thinning hair, a gray beard and rimless glasses, Dr. Levin looks every bit
the psychiatrist pictured for decades in New Yorker cartoons. His office, just
above Dog Daze Canine Hair Designs in this suburb of Philadelphia, has matching
leather chairs, and African masks and a moose head on the wall. But there is no
couch or daybed; Dr. Levin has neither the time nor the space for patients to
lie down anymore.
On a recent day, a 50-year-old man visited Dr. Levin to get his prescriptions
renewed, an encounter that took about 12 minutes.
Two years ago, the man developed rheumatoid arthritis and became severely
depressed. His family doctor prescribed an antidepressant, to no effect. He went
on medical leave from his job at an insurance company, withdrew to his basement
and rarely ventured out.
“I became like a bear hibernating,” he said.
Missing the Intrigue
He looked for a psychiatrist who would provide talk therapy, write prescriptions
if needed and accept his insurance. He found none. He settled on Dr. Levin, who
persuaded him to get talk therapy from a psychologist and spent months adjusting
a mix of medications that now includes different antidepressants and an
antipsychotic. The man eventually returned to work and now goes out to movies
and friends’ houses.
The man’s recovery has been gratifying for Dr. Levin, but the brevity of his
appointments — like those of all of his patients — leaves him unfulfilled.
“I miss the mystery and intrigue of psychotherapy,” he said. “Now I feel like a
good Volkswagen mechanic.”
“I’m good at it,” Dr. Levin went on, “but there’s not a lot to master in
medications. It’s like ‘2001: A Space Odyssey,’ where you had Hal the
supercomputer juxtaposed with the ape with the bone. I feel like I’m the ape
with the bone now.”
The switch from talk therapy to medications has swept psychiatric practices and
hospitals, leaving many older psychiatrists feeling unhappy and inadequate. A
2005 government survey found that just 11 percent of psychiatrists provided talk
therapy to all patients, a share that had been falling for years and has most
likely fallen more since. Psychiatric hospitals that once offered patients
months of talk therapy now discharge them within days with only pills.
Recent studies suggest that talk therapy may be as good as or better than drugs
in the treatment of depression, but fewer than half of depressed patients now
get such therapy compared with the vast majority 20 years ago. Insurance company
reimbursement rates and policies that discourage talk therapy are part of the
reason. A psychiatrist can earn $150 for three 15-minute medication visits
compared with $90 for a 45-minute talk therapy session.
Competition from psychologists and social workers — who unlike psychiatrists do
not attend medical school, so they can often afford to charge less — is the
reason that talk therapy is priced at a lower rate. There is no evidence that
psychiatrists provide higher quality talk therapy than psychologists or social
workers.
Of course, there are thousands of psychiatrists who still offer talk therapy to
all their patients, but they care mostly for the worried wealthy who pay in
cash. In New York City, for instance, a select group of psychiatrists charge
$600 or more per hour to treat investment bankers, and top child psychiatrists
charge $2,000 and more for initial evaluations.
When he started in psychiatry, Dr. Levin kept his own schedule in a spiral
notebook and paid college students to spend four hours a month sending out
bills. But in 1985, he started a series of jobs in hospitals and did not return
to full-time private practice until 2000, when he and more than a dozen other
psychiatrists with whom he had worked were shocked to learn that insurers would
no longer pay what they had planned to charge for talk therapy.
“At first, all of us held steadfast, saying we spent years learning the craft of
psychotherapy and weren’t relinquishing it because of parsimonious policies by
managed care,” Dr. Levin said. “But one by one, we accepted that that craft was
no longer economically viable. Most of us had kids in college. And to have your
income reduced that dramatically was a shock to all of us. It took me at least
five years to emotionally accept that I was never going back to doing what I did
before and what I loved.”
He could have accepted less money and could have provided time to patients even
when insurers did not pay, but, he said, “I want to retire with the lifestyle
that my wife and I have been living for the last 40 years.”
“Nobody wants to go backwards, moneywise, in their career,” he said. “Would
you?”
Dr. Levin would not reveal his income. In 2009, the median annual compensation
for psychiatrists was about $191,000, according to surveys by a medical trade
group. To maintain their incomes, physicians often respond to fee cuts by
increasing the volume of services they provide, but psychiatrists rarely earn
enough to compensate for their additional training. Most would have been better
off financially choosing other medical specialties.
Dr. Louisa Lance, a former colleague of Dr. Levin’s, practices the old style of
psychiatry from an office next to her house, 14 miles from Dr. Levin’s office.
She sees new patients for 90 minutes and schedules follow-up appointments for 45
minutes. Everyone gets talk therapy. Cutting ties with insurers was frightening
since it meant relying solely on word-of-mouth, rather than referrals within
insurers’ networks, Dr. Lance said, but she cannot imagine seeing patients for
just 15 minutes. She charges $200 for most appointments and treats fewer
patients in a week than Dr. Levin treats in a day.
“Medication is important,” she said, “but it’s the relationship that gets people
better.”
Dr. Levin’s initial efforts to get insurers to reimburse him and persuade his
clients to make their co-payments were less than successful. His office
assistants were so sympathetic to his tearful patients that they often failed to
collect. So in 2004, he begged his wife, Laura Levin — a licensed talk therapist
herself, as a social worker — to take over the business end of the practice.
Ms. Levin created accounting systems, bought two powerful computers, licensed a
computer scheduling program from a nearby hospital and hired independent
contractors to haggle with insurers and call patients to remind them of
appointments. She imposed a variety of fees on patients: $50 for a missed
appointment, $25 for a faxed prescription refill and $10 extra for a missed
co-payment.
As soon as a patient arrives, Ms. Levin asks firmly for a co-payment, which can
be as much as $50. She schedules follow-up appointments without asking for
preferred times or dates because she does not want to spend precious minutes as
patients search their calendars. If patients say they cannot make the
appointments she scheduled, Ms. Levin changes them.
“This is about volume,” she said, “and if we spend two minutes extra or five
minutes extra with every one of 40 patients a day, that means we’re here two
hours longer every day. And we just can’t do it.”
She said that she would like to be more giving of herself, particularly to
patients who are clearly troubled. But she has disciplined herself to confine
her interactions to the business at hand. “The reality is that I’m not the
therapist anymore,” she said, words that echoed her husband’s.
Drawing the Line
Ms. Levin, 63, maintains a lengthy waiting list, and many of the requests are
heartbreaking. On a January day, a pregnant mother of a 3-year-old called to say
that her husband was so depressed he could not rouse himself from bed. Could he
have an immediate appointment? Dr. Levin’s first opening was a month away.
“I get a call like that every day, and I find it really distressing,” Ms. Levin
said. “But do we work 12 hours every day instead of 11? At some point, you have
to make a choice.”
Initial consultations are 45 minutes, while second and later visits are 15. In
those first 45 minutes, Dr. Levin takes extensive medical, psychiatric and
family histories. He was trained to allow patients to tell their stories in
their own unhurried way with few interruptions, but now he asks a rapid-fire
series of questions in something akin to a directed interview. Even so, patients
sometimes fail to tell him their most important symptoms until the end of the
allotted time.
“There was a guy who came in today, a 56-year-old man with a series of business
failures who thinks he has A.D.D.,” or attention deficit disorder, Dr. Levin
said. “So I go through the whole thing and ask a series of questions about
A.D.D., and it’s not until the very end when he says, ‘On Oct. 28, I thought
life was so bad, I was thinking about killing myself.’ ”
With that, Dr. Levin began to consider an entirely different diagnosis from the
man’s pattern of symptoms: excessive worry, irritability, difficulty falling
asleep, muscle tension in his back and shoulders, persistent financial woes, the
early death of his father, the disorganization of his mother.
“The thread that runs throughout this guy’s life is anxiety, not A.D.D. —
although anxiety can impair concentration,” said Dr. Levin, who prescribed an
antidepressant that he hoped would moderate the man’s anxiety. And he pressed
the patient to see a therapist, advice patients frequently ignore. The visit
took 55 minutes, putting Dr. Levin behind schedule.
In 15-minute consultations, Dr. Levin asks for quick updates on sleep, mood,
energy, concentration, appetite, irritability and problems like sexual
dysfunction that can result from psychotropic medications.
“And people want to tell me about what’s going on in their lives as far as
stress,” Dr. Levin said, “and I’m forced to keep saying: ‘I’m not your
therapist. I’m not here to help you figure out how to get along with your boss,
what you do that’s self-defeating, and what alternative choices you have.’ ”
Dr. Levin, wearing no-iron khakis, a button-down blue shirt with no tie, blue
blazer and loafers, had a cheery greeting for his morning patients before
ushering them into his office. Emerging 15 minutes later after each session, he
would walk into Ms. Levin’s adjoining office to pick up the next chart, announce
the name of the patient in the waiting room and usher that person into his
office.
He paused at noon to spend 15 minutes eating an Asian chicken salad with Ramen
noodles. He got halfway through the salad when an urgent call from a patient
made him put down his fork, one of about 20 such calls he gets every day.
By afternoon, he had dispensed with the cheery greetings. At 6 p.m., his waiting
room empty, Dr. Levin heaved a sigh after emerging from his office with his 39th
patient. Then the bell on his entry door tinkled again, and another patient came
up the stairs.
“Oh, I thought I was done,” Dr. Levin said, disappointed. Ms. Levin handed him
the last patient’s chart.
Quick Decisions
The Levins said they did not know how long they could work 11-hour days. “And if
the stock market hadn’t gone down two years ago, we probably wouldn’t be working
this hard now,” Ms. Levin said.
Dr. Levin said that the quality of treatment he offers was poorer than when he
was younger. For instance, he was trained to adopt an unhurried analytic calm
during treatment sessions. “But my office is like a bus station now,” he said.
“How can I have an analytic calm?”
And years ago, he often saw patients 10 or more times before arriving at a
diagnosis. Now, he makes that decision in the first 45-minute visit. “You have
to have a diagnosis to get paid,” he said with a shrug. “I play the game.”
In interviews, six of Dr. Levin’s patients — their identities, like those of the
other patients, are being withheld to protect their privacy — said they liked
him despite the brief visits. “I don’t need a half-hour or an hour to talk,”
said a stone mason who has panic attacks and depression and is prescribed an
antidepressant. “Just give me some medication, and that’s it. I’m O.K.”
Another patient, a licensed therapist who has post-partum depression worsened by
several miscarriages, said she sees Dr. Levin every four weeks, which is as
often as her insurer will pay for the visits. Dr. Levin has prescribed
antidepressants as well as drugs to combat anxiety. She also sees a therapist,
“and it’s really, really been helping me, especially with my anxiety,” she said.
She said she likes Dr. Levin and feels that he listens to her.
Dr. Levin expressed some astonishment that his patients admire him as much as
they do.
“The sad thing is that I’m very important to them, but I barely know them,” he
said. “I feel shame about that, but that’s probably because I was trained in a
different era.”
The Levins’s youngest son, Matthew, is now training to be a psychiatrist, and
Dr. Donald Levin said he hoped that his son would not feel his ambivalence about
their profession since he will not have experienced an era when psychiatrists
lavished time on every patient. Before the 1920s, many psychiatrists were stuck
in asylums treating confined patients covered in filth, so most of the 20th
century was unusually good for the profession.
In a telephone interview from the University of California, Irvine, where he is
completing the last of his training to become a child and adolescent
psychiatrist, Dr. Matthew Levin said, “I’m concerned that I may be put in a
position where I’d be forced to sacrifice patient care to make a living, and I’m
hoping to avoid that.”
Talk Doesn’t Pay, So
Psychiatry Turns to Drug Therapy, NYT, 5.3.2011,
http://www.nytimes.com/2011/03/06/health/policy/06doctors.html
Edwin Kilbourne, Flu Vaccine Expert, Dies at 90
February 24, 2011
The New York Times
By DOUGLAS MARTIN
Dr. Edwin D. Kilbourne, a medical researcher who figured out how to outwit
fast-evolving flu germs, developing a new vaccine each year by intermingling
genes of different disease strains, died Monday in Branford, Conn. He was 90.
His family announced the death. He lived in Madison, Conn.
For all his prestigious discoveries, awards and positions, Dr. Kilbourne had his
greatest visibility during the swine flu epidemic of 1976. When a soldier died
at Fort Dix, N.J., after being infected by a particularly virulent flu virus,
Dr. Kilbourne wrote an Op-Ed article in The New York Times warning of a
worldwide flu pandemic, and personally led in developing a vaccine to meet its
challenge.
President Gerald R. Ford ordered 200 million doses of the vaccine to be
administered to that many Americans. Dr. Kilbourne was a principal adviser to
the president on the program. But even as the disease seemed to subside on its
own, several hundred people who received shots contracted a kind of paralysis.
Some died.
Time magazine asserted that “election-year fever” had prompted the president to
move quickly, while The Times called Mr. Ford’s scientific advisers
“panicmongers.” The program was stopped after 43 million vaccinations.
A causative connection between the vaccinations and the paralytic syndrome was
never proved. And Dr. Kilbourne remained convinced that the mass vaccinations
were the right policy, pointing out that the virus that killed the soldier bore
a sinister resemblance to the pandemic of 1918-19, which infected two billion
people around the world and killed 20 million to 40 million. He also warned that
the disease could be hibernating, which he had proved it could do.
“Better a vaccine without an epidemic than an epidemic without a vaccine,” he
said years later. He called the episode “my 15 minutes of infamy.”
Although Dr. Kilbourne never stopped believing that Mr. Ford’s aggressive
actions were warranted, only 230 cases of flu were diagnosed at Fort Dix, and
none elsewhere.
Of the 43 million who got flu shots, 535 came down with the paralytic syndrome
known as Guillain-Barré; 23 of them died.
Dr. Kilbourne’s early research examined links between hormones and viruses, but
it was his work on the flu that earned him global note as early as the
mid-1950s. His goal was to find weapons to combat the flu virus comparable to
the way penicillin fights bacterial infections.
He was up against one of the most fickle, enigmatic, persistent microbes to
attack man or beast. These microbes are capable of changing their surface
characteristics to elude barriers the body has erected against them. Dr.
Kilbourne’s solution was to mix, or “recombine,” the genes of different strains
of the virus to “persuade” the body to come up with new defenses.
“This accomplishment represents the first deliberate genetic engineering of any
vaccine,” the New York Academy of Medicine said in presenting Dr. Kilbourne with
its highest award in 1983. For years after, he created annual versions of flu
vaccine targeted at emerging viruses.
In 1973, Dr. Kilbourne proposed that worldwide epidemics might be terrestrial
“Andromeda strains” coming to man from the barnyard and then retreating to await
the next great outbreak. “The Andromeda Strain” in Michael Crichton’s novel of
that name is an organism from outer space that Earth is not prepared to handle.
In delivering the R. E. Dyer lecture to the National Institutes of Health in
1973, Dr. Kilbourne suggested that two conditions must be met for a new viral
strain to go from swine or other animals to man. One was the random
recombination of a virus, making it infectious to man. The other was an
ecological niche for the virus in a human population unprepared to fight back.
“If my hypothesis is correct,” he said, “the pandemic viruses of tomorrow and of
remote yesterdays may already exist in our domestic animals today.”
Edwin Dennis Kilbourne was born on July 10, 1920, in Buffalo. He graduated from
Cornell University in 1942 and Cornell Medical College in 1944. For the next two
years he served in the Army, where he became intrigued with influenza while
treating soldiers.
He next worked as a researcher at the Rockefeller Institute before working at
four medical schools: Tulane, Cornell, Mount Sinai (as chairman of the
microbiology department) and New York Medical College.
Dr. Kilbourne is survived by his wife of 58 years, the former Joy Schmid; his
sister, Sylvia Hosie; his half-sister, Lynn Norton; his sons, Edwin, Richard,
Christopher and Paul; and eight grandchildren.
Over the desk in Dr. Kilbourne’s laboratory, the most prominent award, obscuring
honors like his membership in the National Academy of Sciences, was a plaque
honoring his contribution to his team’s 1988-89 victory in a men’s bowling
league in Ho-Ho-Kus, N.J.
He was also a published poet, devoted to extolling the bizarre mating habits of
animals like hairy-legged fruit flies. A paean to the bighorn ram illustrates:
His wooly wooing is neither smooth nor is it unctuous,
And therefore can be fairly termed rambunctious.
Edwin Kilbourne, Flu
Vaccine Expert, Dies at 90, NYT, 24.2.2011,
http://www.nytimes.com/2011/02/25/us/politics/25kilbourne.html
A Bush Rule on Providers of Abortions Is Revised
February 18, 2011
The New York Times
By ROBERT PEAR
WASHINGTON — The Obama administration on Friday rescinded most of
a 2008 rule that granted sweeping protections to health care providers who
opposed abortion, sterilization and other medical procedures on religious or
moral grounds.
Kathleen Sebelius, the secretary of health and human services, said the rule,
issued in the last days of the Bush administration, could “negatively impact
patient access to contraception and certain other medical services.”
Federal laws make clear that health care providers cannot be compelled to
perform or assist in an abortion, Ms. Sebelius said. The Bush rule went far
beyond these laws and upset the balance between patients’ rights to obtain
health care and “the conscience rights of health care providers,” she added.
The Obama administration retained and updated part of the 2008 rule that
established procedures to investigate complaints from health care workers who
believe they have been subjected to discrimination or coercion because of their
“religious beliefs or moral convictions.”
Although the Bush rule is still on the books, the Obama administration has not
enforced it. Eight states and several organizations filed a lawsuit in Federal
District Court in Connecticut challenging the 2008 rule as vague and overly
broad. The court suspended proceedings in the case, pending issuance of the rule
published Friday.
The Roman Catholic Church and some Republicans, like Representative Joe Pitts of
Pennsylvania, criticized the Obama administration’s decision to revoke the Bush
rule. But advocates for abortion rights welcomed it.
“The administration’s action today is cause for disappointment,” said Deirdre A.
McQuade, a spokeswoman for the Pro-Life Secretariat at the United States
Conference of Catholic Bishops.
Senator Richard Blumenthal, Democrat of Connecticut, said: “I applaud the Obama
administration for ensuring that women will have access to the information and
services they need while still protecting the conscience rights of health care
providers. The Bush rule clearly went too far and threatened the health and
well-being of millions of patients.”
The 2008 rule provoked a torrent of criticism from doctors, pharmacists,
hospitals and state officials. Pharmacies said the rule would allow their
employees to refuse to fill prescriptions for contraceptives. State officials
said the rule could void state laws that require insurance plans to cover
contraceptives and require hospitals to offer emergency contraception to rape
victims.
Clare M. Coleman, president of the National Family Planning and Reproductive
Health Association, which represents hundreds of family planning clinics, said
President Obama was rescinding “the most harmful elements” of the Bush rule.
The Obama administration said the 2008 rule might have mistakenly suggested that
health care providers could refuse to treat entire groups of people on account
of the providers’ religious or moral beliefs.
Federal laws provide no protection for such refusals, the administration said.
The bishops conference and the Catholic Health Association, representing
Catholic hospitals, had supported the Bush rule as a way to protect health care
providers against pressure to perform abortions.
Sister Carol Keehan, president of the Catholic Health Association, said that in
recent years “we have seen a variety of efforts to force Catholic and other
health care providers to perform or refer for abortions and sterilizations.”
In response to such concerns, the Obama administration said, “Roman Catholic
hospitals will have the same statutory protections afforded to them for decades”
because the laws were not affected by the cancellation of the Bush rule.
A Bush Rule on Providers
of Abortions Is Revised, NYT, 18.2.2011,
http://www.nytimes.com/2011/02/19/health/policy/19health.html
Clearing the Fog in Nursing Homes
February 15, 2011
11:10 am
The New York Times
By PAULA SPAN
The woman, who was in her 90s, had lived for several years at the Ecumen
Sunrise nursing home in Two Harbors, Minn., where the staff had grown accustomed
to her grimaces and wordless cries. She took a potent cocktail of three
psychotropic drugs: Ativan for anxiety and the antipsychotic Risperdal to calm
her, plus an antidepressant. In all the time she’d lived at Sunrise, she hadn’t
spoken. It wasn’t clear whether she could recognize her children when they came
to visit.
Belinda Day Saylor Eva Lanigan, right, director of nursing at the Ecumen nursing
home in Two Harbors, Minn., with a resident, Marjorie Labrie, 94.The Two Harbors
home happened to be where Ecumen, which operates 16 nonprofit Minnesota nursing
homes, was preparing an experiment to see if behavioral rather than
pharmacological approaches could help wean residents off antipsychotic
medications. They called it the Awakenings program.
“What’s people’s biggest fear? Being a ‘zombie’ in a nursing home,” said Laurel
Baxter, the Awakenings project manager.
Any visitor can see what she means. Even in quality nursing homes, some
residents sit impassively in wheelchairs or nod off in front of televisions,
apparently unable to interact with others or to summon much interest in their
lives. Nursing home reformers and regulators have long believed that this
disengagement results in part from the overuse of psychotropic medication to
quell the troublesome behaviors that can accompany dementia — yelling,
wandering, aggression, resisting care. For nearly 25 years, federal law has
required that psychotropic drugs (which critics call “chemical restraints”) be
used only when necessary to ensure the safety of a resident or those around her.
The drugs can cause serious side effects. Since 2008, the Food and Drug
Administration has required a so-called black box warnings on their packaging,
cautioning that they pose an increased mortality risk for elderly patients.
Nevertheless, a national survey reported that in 2004 about a quarter of nursing
home residents were receiving antipsychotic drugs. (Among the antipsychotic
drugs most commonly used in nursing homes are Risperdal, Seroquel and Zyprexa.)
Though they may be prescribed less frequently following the F.D.A.’s warnings,
these drugs are still overused in long-term care, said Dr. Mark Lachs, chief of
geriatrics at Weill Cornell Medical College. And once the pills are prescribed,
residents keep taking them. “They get perpetualized, like insulin,” he told me,
even though the behaviors they’re meant to soothe may wane anyway as dementia
progresses.
“If a place is understaffed, if it takes particularly unruly patients, you can
see how it happens,” Dr. Lachs added. “Behavioral interventions are far more
time-consuming than giving a pill.”
Nevertheless, Ecumen’s Awakenings project emphasizes nondrug responses.
“Medications have a place, but that shouldn’t be the first thing you try,” said
Eva Lanigan, director of nursing at the Two Harbors facility.
So the home trained its entire staff (housekeepers, cooks, dining room servers,
everyone) in a variety of tools to calm and reassure its 55 residents: exercise,
activities, music, massage, aromatherapy. It taught people the kind of
conversation known as “redirecting” — listening to elders and responding to them
without insisting on facts that those with dementia can’t absorb or won’t
recall.
“The hands-on, caring part is the most important,” Ms. Lanigan said. “Sometimes,
people just want a hug. You sit and hold their hand.”
At the same time, consulting with a geriatric psychiatrist and a pharmacist, the
home began gradually reducing the doses of antipsychotics and antidepressants
for patients whose families agreed. Among them: the woman with the mysterious
cries.
As Dr. Lachs pointed out, behavioral interventions are labor-intensive. Two
Harbors hired an additional nurse to oversee those efforts, and Ms. Lanigan was
available to answer staff questions around the clock. Ecumen estimates that
introducing the program to a 60-bed nursing home cost an additional $75,000 a
year for two full-time employees.
The results startled even the believers, however. Every resident on
antipsychotics (about 10) was able to stop taking them, and 30 to 50 percent of
those taking antidepressants also did well without them. When drugs still seemed
necessary, “we tried to reduce them to the lowest dose possible,” Ms. Lanigan
said.
Encouraged, Ecumen has introduced the Awakenings program to its 15 other nursing
homes, using a $3.8 million, three-year grant from the state of Minnesota. “I
believe we may learn that spending a little time now with a resident, preventing
the use of psychiatric medications and their side effects, you’ll save time and
money in the long run,” said Ms. Baxter, the project manager. “I’m optimistic.”
Of course, you can’t tell how well nondrug approaches work based on one
facility’s outcomes. “We know how to reduce behavior problems and mood issues in
controlled clinical trials,” said Kimberly Van Haitsma, a senior research
scientist at the Polisher Research Institute in Philadelphia. “The actual nuts
and bolts of how do you do this and keep it in place — over not weeks or months,
but years — is a question the field is struggling with.” Turnover among both
staff and residents is high in nursing homes, she pointed out.
But with reduced medications, the woman at the Two Harbors home did seem to
awaken. She was able to speak — haltingly and not always understandably, but
enough to communicate. And what she let Ms. Lanigan know, after years of being
virtually nonverbal, was that she was suffering physical pain, the cause of her
crying out.
It took doctors a while to find effective medications for her nerve condition,
but they were eventually able to make her more comfortable without further
fogging her mind. She stopped taking psychotropic drugs altogether.
None of this can halt dementia; it’s a terminal disease, and it took this
resident’s life last year. But in her final months, she smiled and played
balloon volleyball with other residents and could say she felt fine or was
hungry.
“She engaged more. Her family came to help her eat,” Ms. Lanigan said. “It was a
big change.”
Paula Span is the author of “When the Time Comes: Families With Aging Parents
Share Their Struggles and Solutions.”
Clearing the Fog in
Nursing Homes, NYT, 15.2.2011,
http://newoldage.blogs.nytimes.com/2011/02/15/clearing-the-fog-in-nursing-homes/
Lymph Node Study Shakes Pillar of Breast Cancer Care
February 8, 2011
The New York Times
By DENISE GRADY
A new study finds that many women with early breast cancer do not need a
painful procedure that has long been routine: removal of cancerous lymph nodes
from the armpit.
The discovery turns standard medical practice on its head. Surgeons have been
removing lymph nodes from under the arms of breast cancer patients for 100
years, believing it would prolong women’s lives by keeping the cancer from
spreading or coming back.
Now, researchers report that for women who meet certain criteria — about 20
percent of patients, or 40,000 women a year in the United States — taking out
cancerous nodes has no advantage. It does not change the treatment plan, improve
survival or make the cancer less likely to recur. And it can cause complications
like infection and lymphedema, a chronic swelling in the arm that ranges from
mild to disabling.
Removing the cancerous lymph nodes proved unnecessary because the women in the
study had chemotherapy and radiation, which probably wiped out any disease in
the nodes, the researchers said. Those treatments are now standard for women
with breast cancer in the lymph nodes, based on the realization that once the
disease reaches the nodes, it has the potential to spread to vital organs and
cannot be eliminated by surgery alone.
Experts say that the new findings, combined with similar ones from earlier
studies, should change medical practice for many patients. Some centers have
already acted on the new information. Memorial Sloan-Kettering Cancer Center in
Manhattan changed its practice in September, because doctors knew the study
results before they were published. But more widespread change may take time,
experts say, because the belief in removing nodes is so deeply ingrained.
“This is such a radical change in thought that it’s been hard for many people to
get their heads around it,” said Dr. Monica Morrow, chief of the breast service
at Sloan-Kettering and an author of the study, which is being published
Wednesday in The Journal of the American Medical Association. The National
Cancer Institute paid for the study.
Doctors and patients alike find it easy to accept more cancer treatment on the
basis of a study, Dr. Morrow said, but get scared when the data favor less
treatment.
The new findings are part of a trend to move away from radical surgery for
breast cancer. Rates of mastectomy, removal of the whole breast, began declining
in the 1980s after studies found that for many patients, survival rates after
lumpectomy and radiation were just as good as those after mastectomy.
The trend reflects an evolving understanding of breast cancer. In decades past,
there was a belief that surgery could “get it all” — eradicate the cancer before
it could spread to organs and bones. But research has found that breast cancer
can begin to spread early, even when tumors are small, leaving microscopic
traces of the disease after surgery.
The modern approach is to cut out obvious tumors — because lumps big enough to
detect may be too dense for drugs and radiation to destroy — and to use
radiation and chemotherapy to wipe out microscopic disease in other places.
But doctors have continued to think that even microscopic disease in the lymph
nodes should be cut out to improve the odds of survival. And until recently,
they counted cancerous lymph nodes to gauge the severity of the disease and
choose chemotherapy. But now the number is not so often used to determine drug
treatment, doctors say. What matters more is whether the disease has reached any
nodes at all. If any are positive, the disease could become deadly. Chemotherapy
is recommended, and the drugs are the same, no matter how many nodes are
involved.
The new results do not apply to all patients, only to women whose disease and
treatment meet the criteria in the study.
The tumors were early, at clinical stage T1 or T2, meaning less than two inches
across. Biopsies of one or two armpit nodes had found cancer, but the nodes were
not enlarged enough to be felt during an exam, and the cancer had not spread
anywhere else. The women had lumpectomies, and most also had radiation to the
entire breast, and chemotherapy or hormone-blocking drugs, or both.
The study, at 115 medical centers, included 891 patients. Their median age was
in the mid-50s, and they were followed for a median of 6.3 years.
After the initial node biopsy, the women were assigned at random to have 10 or
more additional nodes removed, or to leave the nodes alone. In 27 percent of the
women who had additional nodes removed, those nodes were cancerous. But over
time, the two groups had no difference in survival: more than 90 percent
survived at least five years. Recurrence rates in the armpit were also similar,
less than 1 percent. If breast cancer is going to recur under the arm, it tends
to do so early, so the follow-up period was long enough, the researchers said.
One potential weakness in the study is that there was not complete follow-up
information on 166 women, about equal numbers from each group. The researchers
said that did not affect the results. A statistician who was not part of the
study said the missing information should have been discussed further, but
probably did not have an important impact.
It is not known whether the findings also apply to women who do not have
radiation and chemotherapy, or to those who have only part of the breast
irradiated. Nor is it known whether the findings could be applied to other types
of cancer.
The results mean that women like those in the study will still have to have at
least one lymph node removed, to look for cancer and decide whether they will
need more treatment. But taking out just one or a few nodes should be enough.
Dr. Armando E. Giuliano, the lead author of the study and the chief of surgical
oncology at the John Wayne Cancer Institute at St. John’s Health Center in Santa
Monica, Calif., said: “It shouldn’t come as a big surprise, but it will. It’s
hard for us as surgeons and medical oncologists and radiation oncologists to
accept that you don’t have to remove the nodes in the armpit.”
Dr. Grant W. Carlson, a professor of surgery at the Winship Cancer Institute at
Emory University, and the author of an editorial accompanying the study, said
that by routinely taking out many nodes, “I have a feeling we’ve been doing a
lot of harm.”
Indeed, women in the study who had the nodes taken out were far more likely (70
percent versus 25 percent) to have complications like infections, abnormal
sensations and fluid collecting in the armpit. They were also more likely to
have lymphedema.
But Dr. Carlson said that some of his colleagues, even after hearing the new
study results, still thought the nodes should be removed.
“The dogma is strong,” he said. “It’s a little frustrating.”
Eventually, he said, genetic testing of breast tumors might be enough to
determine the need for treatment, and eliminate the need for many node biopsies.
Two other breast surgeons not involved with the study said they would take it
seriously.
Dr. Elisa R. Port, the chief of breast surgery at Mount Sinai Medical Center in
Manhattan, said: “It’s a big deal in the world of breast cancer. It’s definitely
practice-changing.”
Dr. Alison Estabrook, the chief of the comprehensive breast center at St.
Luke’s-Roosevelt hospital in New York said surgeons had long been awaiting the
results.
“In the past, surgeons thought our role was to get out all the cancer,” Dr.
Estabrook said. “Now he’s saying we don’t really have to do that.”
But both Dr. Estabrook and Dr. Port said they would still have to make judgment
calls during surgery and remove lymph nodes that looked or felt suspicious.
The new research grew out of efforts in the 1990s to minimize lymph node surgery
in the armpit, called axillary dissection. Surgeons developed a technique called
sentinel node biopsy, in which they injected a dye into the breast and then
removed just one or a few nodes that the dye reached first, on the theory that
if the tumor was spreading, cancer cells would show up in those nodes. If there
was no cancer, no more nodes were taken. But if there were cancer cells, the
surgeon would cut out more nodes.
Although the technique spared many women, many others with positive nodes still
had extensive cutting in the armpit, and suffered from side effects.
“Women really dread the axillary dissection,” Dr. Giuliano said. “They fear
lymphedema. There’s numbness, shoulder pain, and some have limitation of motion.
There are a fair number of serious complications. Women know it.”
After armpit surgery, 20 percent to 30 percent of women develop lymphedema, Dr.
Port said, and radiation may increase the rate to 40 percent to 50 percent.
Physical therapy can help, but there is no cure.
The complications — and the fact that there was no proof that removing the nodes
prolonged survival — inspired Dr. Giuliano to compare women with and without
axillary dissection. Some doctors objected. They were so sure cancerous nodes
had to come out that they said the study was unethical and would endanger women.
“Some prominent institutions wouldn’t even take part in it,” Dr. Giuliano said,
though he declined to name them. “They’re very supportive now. We don’t want to
hurt their feelings. They’ve seen the light.”
Lymph Node Study Shakes
Pillar of Breast Cancer Care, NYT, 8.2.2011,
http://www.nytimes.com/2011/02/09/health/research/09breast.html
Latest Hidden Video by Abortion Foes Shows Bronx Clinic of
Planned Parenthood
February 8, 2011
The New York Times
By ANEMONA HARTOCOLLIS
An anti-abortion group released a videotape on Tuesday of a man whom the
group said was posing as a pimp and a woman who was posing as a prostitute on a
visit to a Planned Parenthood clinic in the Bronx. They appear to get
information from a receptionist about how to obtain abortions and treatment for
sexually transmitted diseases for under-age sex workers.
The videotape was the sixth released by the group, Live Action, of undercover
visits to Planned Parenthood; the others were made at a clinic in New Jersey and
four locations in Virginia. Its release comes as anti-abortion advocates and
their allies in Congress are trying to cut off money for Planned Parenthood,
which provides family planning, contraception and abortion.
Lila Rose, the president of Live Action, which is based in San Jose, Calif.,
said Tuesday that her group had gone after Planned Parenthood because “they’re
the biggest abortion chain in the country.” She said the tape showed that
Planned Parenthood used promises of confidentiality to cover up sex trafficking.
Planned Parenthood of New York City released a statement saying that Live Action
was making “false claims” as part of a political agenda.
“These tapes are part of a nationwide campaign by this group,” the statement
said. “Unlike other publicized tapes, the hoax patients in New York were not
able to get beyond the reception desk for a private consultation.”
Joan Malin, president of Planned Parenthood of New York City, noted that the man
and woman in the video were both adults. She said that if under-age women had
come into the clinic, they would have been screened for violent or abusive
relationships and referred to any necessary services.
“Under New York State law, we are not required to report criminal activity,” Ms.
Malin said. “We are required to report anything we believe is child abuse or
neglect by a parent or guardian, which we do.”
Roger Rathman, a spokesman for Planned Parenthood, said Tuesday that the
organization believed the tape had been doctored to add the words “sex work” and
“sex worker,” and that the two staff members interviewed on camera — a
receptionist and a supervisor — had told the Federal Bureau of Investigation
they did not hear those words.
Ms. Rose, the Live Action president, denied the doctoring claim.
The Live Action Web site shows two versions of the tape, a highly condensed
version and a longer one. The short version shows what appears to be the man and
woman walking toward a clinic, wearing summer clothing, even though the visit to
the Bronx clinic was in the midst of a snowy January. Ms. Rose acknowledged that
the introduction was shot elsewhere.
On the video, a man and a woman — their faces never visible — enter the clinic,
apparently carrying a hidden camera.
A woman who appears to be a receptionist leads them through metal detectors.
Standing in a hall, the man says in a whispery voice that he is wondering “about
testing for the both of us.” The receptionist assumes he is talking about HIV
testing. The man continues: “We’re involved in sex work. We have some other
girls that we manage and work with that they’re gonna need testing as well.”
The receptionist says that everything is confidential and that “they don’t have
to tell anybody what it is that they do.” She says the clinic treats people as
young as 13. At this point the woman posing as a prostitute interjects that
“some of them are 14 and 15.”
The man asks whether he could “sign off as a guardian,” and the receptionist
explains that the clinic does not ask for a guardian’s signature. Under New York
law, minors can get an abortion without parental permission.
Although Live Action describes the couple as posing as a pimp and a prostitute,
they are not heard calling themselves such on the tape.
Planned Parenthood fired an office manager of a New Jersey clinic who was caught
on one video encouraging the pimp to have the girls lie about their ages. The
group ordered retraining for staff members across the country.
Nate Schweber contributed reporting.
Latest Hidden Video by
Abortion Foes Shows Bronx Clinic of Planned Parenthood, NYT, 8.2.2011,
http://www.nytimes.com/2011/02/09/nyregion/09sting.html
On Health Care, Justice Will Prevail
February 7, 2011
The New York Times
By LAURENCE H. TRIBE
Cambridge, Mass.
THE lawsuits challenging the individual mandate in the health care law,
including one in which a federal district judge last week called the law
unconstitutional, will ultimately be resolved by the Supreme Court, and pundits
are already making bets on how the justices will vote.
But the predictions of a partisan 5-4 split rest on a misunderstanding of the
court and the Constitution. The constitutionality of the health care law is not
one of those novel, one-off issues, like the outcome of the 2000 presidential
election, that have at times created the impression of Supreme Court justices as
political actors rather than legal analysts.
Since the New Deal, the court has consistently held that Congress has broad
constitutional power to regulate interstate commerce. This includes authority
over not just goods moving across state lines, but also the economic choices of
individuals within states that have significant effects on interstate markets.
By that standard, this law’s constitutionality is open and shut. Does anyone
doubt that the multitrillion-dollar health insurance industry is an interstate
market that Congress has the power to regulate?
Many new provisions in the law, like the ban on discrimination based on
pre-existing conditions, are also undeniably permissible. But they would be
undermined if healthy or risk-prone individuals could opt out of insurance,
which could lead to unacceptably high premiums for those remaining in the pool.
For the system to work, all individuals — healthy and sick, risk-prone and
risk-averse — must participate to the extent of their economic ability.
In this regard, the health care law is little different from Social Security.
The court unanimously recognized in 1982 that it would be “difficult, if not
impossible” to maintain the financial soundness of a Social Security system from
which people could opt out. The same analysis holds here: by restricting certain
economic choices of individuals, we ensure the vitality of a regulatory regime
clearly within Congress’s power to establish.
The justices aren’t likely to be misled by the reasoning that prompted two of
the four federal courts that have ruled on this legislation to invalidate it on
the theory that Congress is entitled to regulate only economic “activity,” not
“inactivity,” like the decision not to purchase insurance. This distinction is
illusory. Individuals who don’t purchase insurance they can afford have made a
choice to take a free ride on the health care system. They know that if they
need emergency-room care that they can’t pay for, the public will pick up the
tab. This conscious choice carries serious economic consequences for the
national health care market, which makes it a proper subject for federal
regulation.
Even if the interstate commerce clause did not suffice to uphold mandatory
insurance, the even broader power of Congress to impose taxes would surely do
so. After all, the individual mandate is enforced through taxation, even if
supporters have been reluctant to point that out.
Given the clear case for the law’s constitutionality, it’s distressing that many
assume its fate will be decided by a partisan, closely divided Supreme Court.
Justice Antonin Scalia, whom some count as a certain vote against the law,
upheld in 2005 Congress’s power to punish those growing marijuana for their own
medical use; a ban on homegrown marijuana, he reasoned, might be deemed
“necessary and proper” to effectively enforce broader federal regulation of
nationwide drug markets. To imagine Justice Scalia would abandon that
fundamental understanding of the Constitution’s necessary and proper clause
because he was appointed by a Republican president is to insult both his
intellect and his integrity.
Justice Anthony Kennedy, whom many unfairly caricature as the “swing vote,”
deserves better as well. Yes, his opinion in the 5-4 decision invalidating the
federal ban on possession of guns near schools is frequently cited by opponents
of the health care law. But that decision in 1995 drew a bright line between
commercial choices, all of which Congress has presumptive power to regulate, and
conduct like gun possession that is not in itself “commercial” or “economic,”
however likely it might be to set off a cascade of economic effects. The
decision about how to pay for health care is a quintessentially commercial
choice in itself, not merely a decision that might have economic consequences.
Only a crude prediction that justices will vote based on politics rather than
principle would lead anybody to imagine that Chief Justice John Roberts or
Justice Samuel Alito would agree with the judges in Florida and Virginia who
have ruled against the health care law. Those judges made the confused assertion
that what is at stake here is a matter of personal liberty — the right not to
purchase what one wishes not to purchase — rather than the reach of national
legislative power in a world where no man is an island.
It would be asking a lot to expect conservative jurists to smuggle into the
commerce clause an unenumerated federal “right” to opt out of the social
contract. If Justice Clarence Thomas can be counted a nearly sure vote against
the health care law, the only reason is that he alone has publicly and
repeatedly stressed his principled disagreement with the whole line of post-1937
cases that interpret Congress’s commerce power broadly.
There is every reason to believe that a strong, nonpartisan majority of justices
will do their constitutional duty, set aside how they might have voted had they
been members of Congress and treat this constitutional challenge for what it is
— a political objection in legal garb.
Laurence H. Tribe, a professor at Harvard Law School, is the author of “The
Invisible Constitution.”
On Health Care, Justice
Will Prevail, NYT, 7.2.2011,
http://www.nytimes.com/2011/02/08/opinion/08tribe.html
Pharmacies Besieged by Addicted Thieves
February 6, 2011
The New York Times
By ABBY GOODNOUGH
BINGHAM, Me. — The orange signs posted throughout Chet Hibbard’s pharmacy
here relay a blunt warning: We Do Not Stock OxyContin.
Mr. Hibbard stopped dispensing the highly addictive painkiller last July, after
two robbers in ski goggles demanded it at knifepoint one afternoon as shocked
customers looked on. It was one in a rash of armed robberies at Maine drugstores
last year, a sharp increase that has rattled pharmacists and put the police on
high alert.
“I want people to know before they even get in the door that we don’t have it,”
Mr. Hibbard said of OxyContin, which the authorities say is the most common
target of pharmacy robberies here. “Outside hiring an armed guard to be in here
24/7, I don’t know what else to do.”
Maine’s problem is especially stark, but it is hardly the only state dealing
with pharmacy robberies, one of the more jarring effects of the prescription
drug abuse epidemic that has left drugstores borrowing heist-prevention tactics
from the more traditional targets, banks. In at least one case, a tiny tracking
device affixed to a bottle let the police easily track a thief after a robbery.
More than 1,800 pharmacy robberies have taken place nationally over the last
three years, typically conducted by young men seeking opioid painkillers and
other drugs to sell or feed their own addictions. The most common targets are
oxycodone (the main ingredient in OxyContin), hydrocodone (the main ingredient
in Vicodin) and Xanax.
The robbers are brazen and desperate. In Rockland, Me., one wielded a machete as
he leapt over a pharmacy counter to snatch the painkiller oxycodone, gulping
some before he fled. In Satellite Beach, Fla., a robber threatened a pharmacist
with a cordless drill last week, and in North Highlands, Calif., a holdup last
summer led to a shootout that left a pharmacy worker dead.
The crime wave has spurred pharmacists to tighten security measures and add ones
they may never have imagined. Many have upgraded their surveillance cameras;
some have installed bulletproof glass and counters high enough to keep would-be
robbers from jumping them, giving these pharmacies the aesthetic of an urban
liquor store. In Tulsa, Okla., where there was a steep increase in drugstore
robberies last year, at least one pharmacist now requires customers to be buzzed
in the door.
Meanwhile, the police are quietly experimenting with new tools. In Lewiston,
Me., last fall, a Rite Aid pharmacist handed a robber who threatened to shoot
her five bottles of OxyContin, including one that contained a tracking device.
According to court records, the device led the police to the suspect’s home on a
rural road shortly after he fled the store. They gathered evidence there,
arrested the suspect a few days later and indicted him last month.
The Drug Enforcement Administration does not routinely investigate reports of
pharmacy robberies, and therefore “it cannot be determined what factors are
contributing to these types of thefts,” a spokeswoman said.
But some local law enforcement officials have been overwhelmed enough by the
incidents to seek help. Thomas Delahanty II, the United States attorney in
Maine, announced recently that the federal authorities would help investigate
the heists from now on and prosecute some of the cases.
Federal charges could bring more prison time, Mr. Delahanty said, describing the
surge in such robberies as “staggering numbers that can’t be ignored.” There
were 21 in Maine last year, according to the D.E.A., up from two in 2008 and
seven in 2009.
In Biddeford, Me., a city of 21,000 that has had seven pharmacy robberies since
December 2009, Roger Beaupre, the police chief, said he was urging the stores to
require customers to remove hoods and sunglasses before entering and to consider
caging in their pharmacy counters.
Police officers there got free training in how to investigate pharmacy heists
last month from Purdue Pharma, the maker of OxyContin. The company also trains
pharmacists on how to prevent robberies and what to do should they fall victim
to one, said Rick Zenuch, its director of law enforcement liaison and education.
“The very first tip we give them is comply, comply, comply,” Mr. Zenuch said.
“Do exactly what the suspect wants, to end the encounter as soon as possible.”
In Washington State, where more than 100 pharmacy robberies have taken place
over the last three years, law enforcement officials say the penalty for
second-degree robbery, when the pharmacist may be threatened but no weapon is
shown, is too weak. Dan Satterberg, the King County prosecutor, said he had
submitted a bill to the Legislature to increase the minimum jail time to three
years from three months.
“Word travels fast on the street about what an easy target the pharmacies are
and how much profit can be made and what small punishment is attached,” Mr.
Satterberg said.
OxyContin goes for $1 a milligram on the street, Mr. Satterberg and other law
enforcement officials said, and the most popular pill is 80 milligrams.
Many pharmacies in Washington have deterred would-be robbers by putting
time-release locks on the safes where they store narcotics and staggering their
inventory, Mr. Satterberg said. Perhaps as a result, the number of armed
robberies at pharmacies there dropped to 23 in 2010 from 49 in 2008, according
to the D.E.A.
Still, Mr. Satterberg said, the threat of robbery has made it difficult for
retail chains in the state to recruit enough pharmacists in recent years.
“They feel very vulnerable when so many people are so desperate to get what they
keep behind those counters,” he said.
In sheer numbers, Florida, Indiana, California, Ohio and Washington have had the
most armed robberies of pharmacies since January 2008, according to the D.E.A.
But Maine, Oklahoma and Oregon had the sharpest increases last year.
All but a handful of the Maine robberies took place at Rite Aid and CVS stores,
some of which were hit multiple times.
In Tulsa, Okla., where pharmacy robberies last year far outpaced bank robberies,
the police said the crimes were now more often committed by gangs who want to
sell the drugs than addicts in search of a fix. Robbers there often demand
Xanax, an anti-anxiety drug, along with opioids, said Sgt. Dave Walker, who runs
the robbery unit of the Tulsa Police Department.
In Bingham, a remote town of about 1,000, the men who robbed Mr. Hibbard’s
pharmacy, E.W. Moore & Son, were caught and sent to prison, as was another
robber who held up the store at gunpoint in 2006. But despite that comforting
fact and the store’s nine surveillance cameras and high-tech alarm system, Mr.
Hibbard and his employees still jump when the place is quiet and they hear
footsteps coming up the ramp, they said.
“I stood right between him and his knife,” said Lori Pratt, a pharmacy
technician, referring to one of the robbers. “I was all ready to go on the
Internet after it happened and get a Taser gun.”
Unlike Mr. Hibbard, Rite Aid has chosen to keep stocking the drugs that are
popular with robbers, said Eric Harkreader, a spokesman. But the company now
limits the amount of certain drugs in stores at any given time.
“If they are going for lots of quantity at once, we don’t want to help them
out,” he said. “But we certainly want to have the prescription available for all
its legitimate purposes.”
In Biddeford, a Rite Aid that was robbed twice last year was struck again last
week. The suspect, who demanded OxyContin and fled into the night, remains at
large.
Pharmacies Besieged by
Addicted Thieves NYT, 6.2.2011,
http://www.nytimes.com/2011/02/07/us/07pharmacies.html
Too Much of a Good Thing
February 4, 2011
The New York Times
When Mayor Michael Bloomberg began his campaign against cigarette smoking
eight years ago, most New Yorkers breathed a sigh of relief. The great indoors —
bars, restaurants, hotels, office buildings — all are now smoke-free by law,
making New York City a healthier place. And, for those already addicted or
tempted, the city offered kits to help people stop smoking and gruesome
television ads to try to keep them from starting.
That antismoking campaign has been a great public service, but now the mayor and
City Council have overreached. The council voted — 36 to 12 — to ban smoking
outdoors in city parks, beaches and even plazas, including in Times Square.
No smoking at the crossroads of the world? The vortex of tourism that brings
smokers and nonsmokers in great numbers? The site of the world’s most famous New
Year’s Eve party, where who knows what goes on? All of this takes the mayor’s
nannying too far, even for those of us who want to avoid the hazards of
secondhand smoke.
Already smokers are forced to huddle outside, these days perched on the city’s
gray, leftover snowdrifts. Starting in early summer, after the mayor signs the
bill into law, they will not be able to stray onto the 14 miles of city beaches
or into the city’s 1,700 parks, not even Central Park or windswept Battery Park.
Instead of smoking on Brighton Beach, what does a smoker do — take a boat out 12
nautical miles into international waters?
Some City Council members wanted to find a less-drastic solution — like having
the ban but establishing smoking areas on the beach or patches of the park. It’s
not great, but it’s better than an all-out ban. Also, the city would have to
provide a lot more receptacles for cigarette butts and enforce antilittering
laws in those areas.
Meanwhile, there is talk that the mayor and the City Council want even more,
like banning smoking near doors of office buildings and apartments. They need to
take a deep breath and remember that we tried prohibition 90 years ago. They
called it a noble experiment. It turned into a civic disaster.
Too Much of a Good
Thing, NYT, 4.2.2011,
http://www.nytimes.com/2011/02/05/opinion/05sat4.html
City’s High Abortion Rate Defies Easy Explanation
February 3, 2011
The New York Times
By ANEMONA HARTOCOLLIS
At a time when evidence suggests that people in New York City are smoking
less, eating better and biking more, one health statistic that has not budged is
the abortion rate.
Two of every five pregnancies in the city end in abortion, a statistic that has
barely changed in more than a decade. At a news conference last month, Timothy
M. Dolan, the Roman Catholic archbishop of New York, called the city’s 41
percent abortion rate “downright chilling,” and on Thursday, State Senator Rubén
Díaz Sr. of the Bronx, an abortion opponent, is holding a community meeting to
discuss the issue. Nationally, the issue is receiving a new round of attention,
with numerous state legislatures and the House of Representatives considering
bills that would add restrictions on abortion, and Planned Parenthood was
recently a target of undercover videos by an anti-abortion group.
But city health officials and groups that support access to abortion say that
behind the 41 percent statistic — nearly twice the national rate — are complex
social and legal factors: fewer obstacles to abortion in state law; the absence
of mandatory sex education in New York City public schools; the ignorance of
people, especially young ones, about where to get affordable birth control; and
the ambivalence of young women living in poverty and in unstable relationships
about when and whether to have children.
And although the percentage of pregnancies that end in abortion is basically
unchanged, a particularly vulnerable group, teenagers, is having fewer babies
and fewer abortions.
The hand-wringing has led to a rare moment of synchronicity between the Catholic
Church and pro-choice women’s groups, as both say they are disturbed that the
rate is so high, but disagree over what to do about it.
“Listening to Archbishop Dolan, I took a little bit of comfort in that he
recognizes it is important to bring this rate down,” said Joan Malin, president
of Planned Parenthood of New York City. But, she added, “The way we think about
these issues is to really step back a bit and say that the major concern or the
underlying issue that we think is so important is the high rate of unintended
pregnancies.”
The issue came to light with the city health department’s recent release of its
annual Vital Statistics report, which showed that 41 percent of pregnancies,
excluding miscarriages, in 2009 ended in abortion.
Health experts say the abortion rate is tied to factors like race and income.
“If you look at the pregnancy rates by race and ethnicity in New York City
versus nationally, they are essentially the same for black and Hispanic
teenagers, and lower for whites,” said Susan Craig, a spokeswoman for the city’s
health department.
There were 126,774 births, 11,620 miscarriages and 87,273 abortions in New York
City in 2009. Despite the contention of some critics that New York, with its
liberal abortion laws, is a destination state for abortion, nonresidents
accounted for only about 7,000 of these abortions. (Factoring out nonresidents
does not alter the 41 percent abortion rate, because 10,000 nonresidents also
gave birth in the city.)
The little-changed abortion rate figure is a commonly cited statistic. But it
masks large changes in fertility among teenagers.
Since 1996, the number of babies born to teenagers has fallen by 39 percent. The
number of abortions has fallen by more than 16 percent, even though the
population of teenagers has risen modestly. Ninety percent of the teenage
mothers were not married, according to health department estimates.
In that age group in 2009, the rate of abortions was strikingly high for blacks
(74 percent), followed by whites (66 percent) and Hispanics (53 percent). The
rate was also very high for Asians (74 percent), though they were much less
likely to become pregnant.
The drop in teenage pregnancies and abortions, however, was not enough to
significantly alter the overall abortion rate. Most abortions, like most
pregnancies, occurred among women in their 20s. Women in their 30s had abortions
29 percent of the time, and women 40 and older about a third of the time.
Unmarried women accounted for 84 percent of abortions in 2009.
New York State law does not place as many restrictions on abortion as laws in
some other states, like requiring parental consent for minors, or requiring
women to undergo counseling that discourages abortion or to go through a waiting
period.
According to Rachel Jones, a senior research associate at the Guttmacher
Institute, which studies reproductive health issues, the high rate of unwed
pregnancy and abortion among poor women is a sign of ambivalence. They are torn,
she said, between the desire to have a baby and the realization that it would be
hard to bring up a child as a single mother.
“In the U.S., most women want to have kids,” Ms. Jones said. “If you don’t have
a lot of money, when is the responsible time to say, Now I want to have a child?
How long are you supposed to put this off?”
That inner conflict could be seen recently in several women coming out of
Planned Parenthood’s Margaret Sanger Center, a family planning and abortion
clinic in Greenwich Village.
A 17-year-old girl there to pick up a friend said she had had an abortion in
May. It was her second; the first was when she was 15. The girl said she
sometimes used condoms. “But I wasn’t using them when I got pregnant,” she said.
“I might use them more now, but I don’t know.” Like the other women outside the
clinic, she asked not to be named to preserve her privacy.
A 20-year-old woman being helped by two male friends said she had her first
abortion at 16, and also had a 7-month-old child. “It was an accident,” the
woman said. “I used a condom every time, but I already have a kid, and I’m not
ready for another one.”
Another woman, who was 22, said she had become pregnant after not using birth
control because a doctor had told her she was infertile. “I’ve always been
against abortion,” the woman, who is white and lives on Staten Island, said.
“But if I had a kid now, it would have a terrible life. I’d rather wait.”
The health department distributes a pocket-size guide to clinics where teenagers
can get medical care and low-cost or free contraception (information that is
also available through the city’s 311 hotline). It has provided training in
issues like protecting confidentiality and dispensing contraception to 50
clinics serving 32,000 teenagers a year in the neighborhoods with the highest
pregnancy rates among teenagers. School-based classes use role-playing to help
teenagers “learn how to negotiate maybe saying, I don’t want to have sex,” said
Deborah Kaplan, assistant commissioner of the health department’s bureau of
maternal, infant and reproductive health.
Condoms are distributed through health offices at every public high school, Ms.
Kaplan said.
Archbishop Dolan agreed to speak out with other religious leaders at a news
conference last month at the invitation of the Chiaroscuro Foundation, an
anti-abortion group coordinated by an investment banker active in conservative
causes, according to the archbishop’s spokesman, Joseph Zwilling.
The archbishop “reaffirmed and was looking to spread the word as well of the
archdiocese’s longstanding commitment that any woman who is pregnant and in need
can come to the Archdiocese of New York for assistance,” Mr. Zwilling said.
On Thursday, Senator Díaz, a minister who, like the archbishop, advocates
abstinence and not condom use, convened a meeting of other Hispanic ministers to
discuss the abortion statistics and urge them to talk to their congregations
about it.
Juliet Linderman contributed reporting.
City’s High Abortion
Rate Defies Easy Explanation, NYT, 3.2.2011,
http://www.nytimes.com/2011/02/04/nyregion/04abortion.html
For Tucson Survivors, Health Care Cost Is Concern
February 3, 2011
The New York Times
By MARC LACEY and SAM DOLNICK
TUCSON — Seconds after gunfire erupted outside a supermarket here last month,
Randy Gardner, one of those struck during the barrage, said another looming
crisis immediately entered his mind.
“I wondered, ‘How much is this going to cost me?’ ” he said. “It was a thought
that went through my head right away.”
Tucson’s medical system quickly swung into action after the shootings, with
ambulances and medical helicopters rushing victims to hospitals where trauma
specialists awaited them. The life-saving treatment the victims received over
the ensuing days carried a heavy cost though, and the bills — the costliest of
which may be in the hundreds of thousands of dollars for Representative
Gabrielle Giffords — are still being tallied.
But despite the fears of some victims, it does not appear that the shooting will
ruin anybody financially. Interviews with victims as well as advocates assisting
them suggest that most, if not all, of the 13 people wounded that morning had
health insurance, and health care providers say they expect insurance companies
to cover the bulk of the medical costs.
On top of that, the fact that federal charges have been filed against Jared L.
Loughner in the shootings means that state victim-compensation money will be
supplemented by federal help. Private charitable efforts to aid victims have
also been created.
Ms. Giffords, who received a bullet wound to the head and was the most gravely
injured of those who survived the shooting, also had probably the best
insurance, a Congressional plan known for its comprehensive coverage that was
held out as a model during last year’s debate over the health care overhaul.
Dr. Peter Rhee, chief trauma surgeon at Tucson’s University Medical Center, has
repeatedly said that Ms. Giffords received the same care there as any other
gunshot victim. “We don’t have time or luxury to ask for insurance cards or to
know if they are a good guy or how they are going to pay,” he said. “We deal
with whoever comes in the door. We don’t know if they are immigrants, if they
are legal, illegal. We just treat them.”
Still, some of those who are following Ms. Giffords’s treatment, including her
speedy transfer from Tucson to a top rehabilitation facility in Houston, can
only wish their health plans were as responsive.
Monique Pomerleau, a mother of three from Northern California, suffered a
traumatic brain injury in a traffic accident last February but has not yet
undergone rehabilitation because her insurer, Health Net of California, said it
lacked such services within the network.. Her family has hired a lawyer to press
the matter and recently received word that a 30-day rehabilitation program had
been approved. A spokesman for the insurer said federal privacy laws prevented
it from commenting on individual patient’s cases.
“We watched the congresswoman’s care and we thought, How marvelous, but there
are real people out there like Monique who don’t get the same possibilities,”
said Lisa Kantor, a lawyer who specializes in challenging insurance companies
and was hired by Ms. Pomerleau’s father, Tom.
After a tragedy like the Tucson shooting, billing is a topic that appears almost
unseemly to raise. But with health costs spiraling, it is one that was on the
minds of some victims, not to mention their care providers.
“We have to recover our costs so that we can provide the service to others,”
said Craig Yale, vice president of corporate development for the Colorado-based
Air Methods Corporation, which operates LifeNet helicopter service in Tucson,
one of three private helicopter operators that were called to the shooting
scene.
At University Medical Center, where the most seriously injured victims were
treated, Misty Hansen, the hospital’s chief financial officer, said she did not
anticipate any problems recovering costs. “It is my expectation that the bills
will be paid and the hospital will be appropriately compensated,” she said.
Declining to discuss the case of individual patients, Ms. Hansen said 5 percent
of patients were “self pay,” which means they lack insurance and are billed
personally.
Even those like Mr. Gardner, who lost a solid health insurance plan when he
retired five years ago and now has a deductible in the $10,000 range, will most
likely benefit from the plethora of special public and private victim funds to
fill gaps in his coverage.
The Federal Bureau of Investigation’s victim assistant fund cannot be used
directly for medical care. But the money was used after the Tucson shooting to
replace the eyeglasses of two injured victims and to fly relatives of victims to
Tucson and the remains of one victim to her home state, said Kathryn Turman,
director of the F.B.I.’s office for victim assistance.
The Safeway supermarket where Mr. Loughner is accused of spraying the crowd with
bullets has begun a fund to aid victims, although company officials have not yet
detailed how the money will be spent. A nonprofit victims rights group based in
Tucson, Homicide Survivors, is similarly raising money on behalf of victims.
“My fund is too small to cover their medical bills,” said Carol Gaxiola, who is
director of the survivors group. “But we’ll be able to pitch in to cover other
costs.”
Besides the ambulance bill ($991.80 and $16.96 a mile for ground transport) and
the hospital expenses, victims could face travel costs if they wish to follow
the federal court proceedings against Mr. Loughner, especially if the trial is
moved out of state.
There are also the costs of funeral expenses for the six people who died, as
well as trauma counselors and loss of wages for the injured.
Mary Reed, who was shot three times that morning, said her insurer, through her
husband’s job at the University of Arizona, had been unusually responsive and
accommodating since the shooting, approving medicines and services in 24 hours,
significantly faster than usual.
One concern she has, though, is whether her 17-year-old daughter, who was at the
scene but was not hit — Ms. Reed threw herself on her daughter to protect her —
will qualify as a victim. Her husband and son were there as well, and they ran
for cover. They are undergoing counseling, but Ms. Reed is uncertain who will
pick up their costs.
Kenneth Dorushka, 63, was struck in the arm by a bullet and is still awaiting
word on how much of his costs will be covered by his insurer, United Healthcare.
“It’s hard to tell because we haven’t gotten any bills yet, so you don’t know
how much they’re going to cover or not,” said Mr. Dorushka, adding that he had
spent about $100 so far on co-payments and other medical costs.
Ron Barber, district director for Ms. Giffords’s Congressional office who was
hit twice in the shooting, said he expected to emerge from the shooting without
any financial cost.
“I was thinking at first about what kind of deductible I’d have to pay, but then
I learned that workers compensation will cover everything,” said Mr. Barber, who
was working when he was shot.
Even as he recovers at home, Mr. Barber said he was trying to ensure that the
shooting does not cause undo financial strain on those affected.
“It’s obvious that those of us who were shot are victims, but there are others,”
he said. “I don’t know anyone who didn’t have medical coverage, but I’m
interested in making sure no one continues to suffer from this.”
Reporting was contributed by Timothy Williams, Jennifer Medina, Ford
Burkhart and Joseph Goldstein.
For Tucson Survivors,
Health Care Cost Is Concern, NYT, 3.2.2011,
http://www.nytimes.com/2011/02/04/us/04tucson.html
Close Look at a Flu Outbreak Upends Some Common Wisdom
February 3, 2011
The New York Times
By NICHOLAS BAKALAR
If you or your child came down with influenza during the H1N1, or swine flu,
outbreak in 2009, it may not have happened the way you thought it did.
A new study of a 2009 epidemic at a school in Pennsylvania has found that
children most likely did not catch it by sitting near an infected classmate, and
that adults who got sick were probably not infected by their own children.
Closing the school after the epidemic was under way did little to slow the rate
of transmission, the study found, and the most common way the disease spread was
a through child’s network of friends.
Researchers learned all this when they studied an outbreak of H1N1 at an
elementary school in a semirural community in spring 2009. They collected data
in real time, while the epidemic was going on.
With this information on exactly who got sick and when, plus data on seating
charts, activities and social networks, they were able to use statistical
techniques to trace the spread of the disease from one victim to the next. Their
report appears online in the Proceedings of the National Academy of Sciences.
The scientists collected data on 370 students from 295 households. Almost 35
percent of the students and more than 15 percent of their household contacts
came down with flu. The most detailed information was gathered from
fourth-graders, the group most affected by the outbreak.
The class and grade structure had a significant effect on transmission rates.
Transmission was 25 times as intensive among classmates as between children in
different grades. And yet sitting next to a student who was infected did not
increase the chances of catching flu.
Social networks were apparently a more significant means of transmission than
seating arrangements. Students were four times as likely to play with children
of the same sex as with those of the opposite sex, and following this pattern,
boys were more likely to catch the flu from other boys, and girls from other
girls.
The progress of the disease from day to day followed these social interactions:
from May 7 to 9, the illness spread mostly among boys; from May 10 to 13 mostly
among girls.
“Our social networks shape disease spread,” said Simon Cauchemez, the lead
author. “And we can quantify the role of social networks.”
Thirty-eight percent of children 6 to 12 were infected, compared with 23 percent
of 11- to 18-year-olds and 13 percent of those older than 18. Adults were only
about half as susceptible as children, but when they got sick they were just as
likely to transmit the virus to others.
The school closed from May 14 to 18, but there was no indication that this
slowed transmission. It may already have been too late — May 14 was the 18th day
of the outbreak, and 27 percent of the students already had symptoms.
The scientists found no difference in transmission rates during the closure and
during the rest of the outbreak. This, they write, confirms earlier studies
showing that a school has to be closed quite early in an epidemic to have any
effect on disease transmission.
Only 1 in 5 adults caught the illness from their own children, and this goes
against one of the most common arguments for closing schools: that it will
prevent the disease from moving from the school to households.
“Here we find that most of the infected adults were not infected by one of the
children in their household,” said Dr. Cauchemez, a research fellow at Imperial
College London. “This information could be used to understand whether it might
be better to close a school, or to close individual classes or grades.”
Other experts were impressed with the work. “I think it’s a nice step,” said Ira
M. Longini Jr., a professor of biostatistics at the Fred Hutchinson Cancer
Research Center in Seattle. “It’s a beautiful analysis of an important dataset.
This virus spreads very fast among school-age children, so the topic is
important.”
Close Look at a Flu
Outbreak Upends Some Common Wisdom, NYT, 3.2.2011,
http://www.nytimes.com/2011/02/08/health/research/08flu.html
Va. to Ask Supreme Court to Rule on Health Law
February 3, 2011
The New York Times
By KEVIN SACK
Virginia’s attorney general announced on Thursday that he hoped to bypass an
initial appellate review by asking the United States Supreme Court to consider
the constitutionality of the Obama health care law on an expedited basis.
Only rarely does the Supreme Court grant such hearings, and it has already
rejected a similar request in another legal challenge to the health care act.
But the commonwealth’s attorney general, Kenneth T. Cuccinelli II, said the
legal and governmental confusion sown by conflicting lower-court opinions
demanded a rapid resolution.
“Currently, state governments and private businesses are being forced to expend
enormous amounts of resources to prepare to implement a law that, in the end,
may be declared unconstitutional,” Mr. Cuccinelli said in a statement.
In December, Mr. Cuccinelli became the first plaintiff to win a challenge to the
health care act, when Judge Henry E. Hudson of Federal District Court in
Richmond, Va., struck down a provision that requires most Americans to obtain
insurance. The judge ruled that the insurance requirement exceeded Congress’s
authority under the Constitution to regulate interstate commerce.
Two other federal judges, including another in Virginia, had previously upheld
the law. Then on Monday, Judge Roger Vinson of Federal District Court in
Pensacola, Fla., joined Judge Hudson in striking down the insurance mandate. But
unlike Judge Hudson, Judge Vinson invalidated the entire law.
The law, enacted last year by a Democratic Congress and signed in March by
President Obama, aims to cover 32 million uninsured Americans by ending insurer
discrimination against those with pre-existing health conditions and by
providing government subsidies to make coverage affordable.
The Justice Department, which is defending the Obama administration in the
health litigation, has already filed a notice of appeal of Judge Hudson’s ruling
in the Court of Appeals for the Fourth Circuit in Richmond. Because of the
geographic distribution of the four lower court rulings, three different courts
of appeal are likely to hear the cases on their way to the Supreme Court.
Tracy Schmaler, a spokeswoman for the Justice Department, said the agency
continued “to believe this case should follow the ordinary course” so that legal
arguments could be fully developed before being presented to the Supreme Court.
She pointed out that the insurance mandate does not take effect until 2014 and
that the Fourth Circuit has already expedited its schedule by setting oral
arguments for May.
The Justice Department also is considering whether to seek a stay of the Florida
decision in order to clarify confusion about whether the health care act remains
in effect in the 26 states that are plaintiffs in the case.
Mr. Cuccinelli said he recognized that an expedited Supreme Court review would
be exceptional. But he said that this case and the others challenging the
constitutionality of the Patient Protection and Affordable Care Act, as the law
is known, were “truly exceptional in their own right.”
In November, the Supreme Curt refused to review another challenge to the health
care act that had been dismissed by a California judge on grounds that the
plaintiffs did not have standing to sue.
Va. to Ask Supreme Court
to Rule on Health Law, NYT, 3.2.2011,
http://www.nytimes.com/2011/02/04/health/policy/04virginia.html
Senate Rejects Repeal of Health Care Law
February 2, 2011
The New York Times
By DAVID M. HERSZENHORN
WASHINGTON — Senate Democrats on Wednesday defeated a bid by Republicans to
repeal last year’s sweeping health care overhaul, as they successfully mounted a
party-line defense of President Obama’s signature domestic policy achievement.
Challenges to the law will continue, however, on Capitol Hill and in the courts,
with the United States Supreme Court ultimately expected to decide if the law is
constitutional.
The vote was 47 to 51, with all Republicans voting unanimously for repeal but
falling 13 votes short of the 60 needed to advance their proposal.
Lawmakers in both parties joined forces, however, to repeal a tax provision in
the law that would impose a huge information-reporting requirement on small
businesses. That vote was 81 to 17, with 34 Democrats and all 47 Republicans in
favor.
Senators Joseph I. Lieberman, independent of Connecticut, and Mark Warner,
Democrat of Virginia, were absent.
Republicans said after the votes that they would persist in their efforts to
overturn the law. Rejecting assertions that the repeal vote was a “futile act,”
Senator John Cornyn of Texas, the chairman of the Republican Senatorial Campaign
Committee, declared, “These are the first steps in a long road that will
culminate in 2012.”
Senator John Thune, Republican of South Dakota and a potential presidential
candidate in 2012, noted that Republicans had just 40 votes when they opposed
the health care bill last year, but that they had 47 as a result of winning
seats in November.
“Elections do have consequences,” Mr. Thune said.
The vote to eliminate the tax provision offered a brief moment of consensus on a
day otherwise characterized by angry partisan disagreement. In the latest
reprise of last year’s fierce debate over the health care law, senators crossed
rhetorical swords for hours of floor debate.
Republicans denounced the overhaul as impeding job creation and giving the
government too big a role in the health care system. Democrats highlighted the
law’s benefits, especially for the uninsured, and noted that the nonpartisan
Congressional Budget Office had projected that the law would reduce future
deficits.
Senator Rand Paul, Republican of Kentucky, who is an ophthalmologist, cited the
law’s requirement that nearly all Americans obtain insurance as evidence that it
was unconstitutional and overly intrusive.
“If you can regulate inactivity, basically the non-act of not buying insurance,
then there is no aspect to our life that would left free from government
regulation and intrusion,” Mr. Paul said. He added, “From my perspective as a
physician, I saw that we already had too much government involvement in health
care.”
But Democrats hit back hard.
“The Republicans’ obsession with repealing the new health reform law is not
based on budgetary considerations,” said Senator Tom Harkin, Democrat of Iowa,
the chairman of the Health, Education, Labor and Pensions Committee. “It is
based strictly on ideology. They oppose the law’s crackdown on abuses by health
insurance companies and they oppose any serious effort by the federal government
to secure health insurance coverage for tens of millions of Americans who
currently have none.”
And Senator Charles E. Schumer of New York, the No. 3 Democrat, lambasted
Republicans for seeking repeal of the law without proposing an alternative.
“If my colleagues on the other side of the aisle said: ‘You know, you’re right.
We have to reduce costs. We have a better way,’ and they offered a bill on the
floor, well maybe we’d take a look at it,” Mr. Schumer said. “But they’re
silent.” He added: “Easy to sit there and say, ‘repeal.’ What would you put in
its place?”
The repeal measure, which was adopted overwhelmingly by the
Republican-controlled House last month, was put forward by the Senate Republican
leader, Mitch McConnell of Kentucky, as an amendment to an aviation industry
bill that is now on the Senate floor.
The willingness of the majority Senate Democrats to allow a vote on the
amendment reflected a deal among leaders of both parties to limit the
parliamentary warfare and ease the procedural stalemates that have bogged down
the Senate in recent years.
The openness to a vote also reflected confidence among Democrats that they would
be able to defeat the amendment.
And they did, challenging the amendment on the grounds that it violated the
budget resolution by increasing the deficit. To overcome that challenge, and win
approval, Mr. McConnell needed the votes of 60 senators.
On the repeal of the tax provision, a similar challenge on budget grounds was
easily surmounted. Republicans had criticized the provision, which would require
businesses to file a 1099 tax form identifying anyone to whom they paid $600 or
more for goods or merchandise in a year. Businesses would also be required to
send copies of the form to their vendors, suppliers and contractors. The House
is expected to support its repeal.
Because the tax provision was expected to result in increased tax revenue,
Democrats had to come up with another way to generate the same money. The plan
that was approved, sponsored by Senator Debbie Stabenow, Democrat of Michigan,
rescinds $44 billion in unspent money appropriated by Congress. But it exempts
the Pentagon, the Department of Veterans Affairs and the Social Security
Administration from those cuts.
Senate Rejects Repeal of
Health Care Law, NYT, 2.2.2011,
http://www.nytimes.com/2011/02/03/health/policy/03congress.html
F.D.A. Declines to Approve Diet Drug
February 1, 2011
The New York Times
By ANDREW POLLACK
The Food and Drug Administration has declined to approve yet another
prescription diet pill, saying the developer must first do a long-term study to
demonstrate that the drug does not raise the risk of heart attacks.
The failure of the drug, known as Contrave, to gain approval was not totally
unexpected. But the requirement that its developer, Orexigen Therapeutics, first
do a study to rule out cardiovascular problems was somewhat unexpected and could
pose a significant obstacle to approval.
The agency’s decision was announced Tuesday morning by Orexigen, a small company
in San Diego. Its shares fell as much as 73 percent in premarket trading.
The rejection of the drug continues a string of setbacks for pharmaceutical
companies trying to develop medical solutions for one of the country’s most
pressing health problems.
The F.D.A. last year turned down two other drugs, lorcaserin from Arena
Pharmaceuticals and Qnexa from Vivus. It also forced the withdrawal from the
market of Abbott Laboratories’ Meridia.
But hopes had been higher that Contrave would win approval or that the F.D.A.
would impose only minor new requirements, delaying approval for a few months.
Unlike the other two drugs, Contrave won an endorsement from an F.D.A. advisory
committee, which voted 13 to 7 in favor of approval in December.
While the committee called for more study of the potential cardiovascular risks
of the drug, it voted 11 to 8 that such a study could be done after the drug was
approved.
“We are surprised and extremely disappointed with the agency’s requirement in
light of the extensive discussion and resulting vote on this topic at the Dec. 7
advisory committee meeting,” Michael A. Narachi, the chief executive of
Orexigen, said in a statement.
Contrave is a combination of two existing drugs that together work to suppress
food cravings, according to the company. One drug, bupropion, is an
antidepressant known by the brand name Wellbutrin; it is also sold as Zyban to
help people quit smoking. The second ingredient, naltrexone, is used to treat
alcohol and drug addiction.
In a conference call with securities analysts Tuesday, Mr. Narachi said the
company planned to meet with the F.D.A. to discuss details about the proposed
study of cardiovascular risks.
In response to questions, Mr. Narachi said the company had not ruled out any
options, including dropping Contrave or seeking approval only outside the United
States.
Orexigen specializes in obesity drugs and has no products on the market yet. It
has another diet drug, Empatic, which seems somewhat more effective than
Contrave, in the middle stages of clinical trials. But Empatic is also a
combination of two existing drugs, one of which is bupropion, raising questions
about whether that drug would also be affected by safety concerns.
The F.D.A. asked for a randomized trial “of sufficient size and duration” to
demonstrate that the cardiovascular risks of Contrave do not exceed the drug’s
benefits, according to a statement Orexigen provided from the letter it received
late Monday from the F.D.A.
The F.D.A. as a rule does not comment on such matters.
Mr. Narachi said Orexigen had about $100 million in cash as of the end of
September but would need to raise more money if it is to conduct the required
trial.
Such a large randomized trial could conceivably take years and involve 10,000
patients or more, experts said at the advisory committee meeting in December.
One member of the committee said that if such a trial were required before
approval it would kill the drug.
And experts have said that if the F.D.A. were to require such a trial for all
diet pills, it would further discourage pharmaceutical companies from trying to
develop obesity drugs. The agency now requires such big cardiovascular risk
trials for diabetes drugs, and small companies, at least, are shying away from
that field.
The F.D.A. has been very cautious about weight loss drugs, in part because there
is the possibility that they will be very widely used, including by people who
are not obese but might want to lose a few pounds. About a third of American
adults are obese and another third merely overweight.
Still it is not clear that the request for the cardiovascular trial represents a
precedent that would be applied to all obesity drugs. In clinical trials,
Contrave raised pulse rates and blood pressure slightly, a warning that it might
increase the risk of heart attacks, strokes or other cardiovascular problems.
Losing weight is supposed to lower the risk of heart attacks and strokes. And
various diet drugs do produce an improvement in risk measures like blood
pressure, cholesterol and blood sugar.
The F.D.A. could be basing its request for a cardiovascular study on the
experience with Meridia, a weight loss drug by Abbott Laboratories that it
approved in 1997 despite signs that it increased blood pressure and heart rate.
Only last year, a large trial ordered by European regulators showed the drug did
raise the risk of heart attacks and stroke in people already prone to
cardiovascular risks.
Abbott argued that such people should not be getting Meridia in the first place.
But the F.D.A. pushed the company to remove the drug from the market.
The possible cardiovascular risks of Orexigen’s Contrave, combined with only
modest effectiveness in helping people lose weight, left the advisory committee
somewhat lukewarm about the drug even as it voted to recommend approval.
“I think they made it by the hair of their chinny chin chin,” Melanie Coffin,
the patient representative on the committee, said during the December meeting.
In four clinical trials involving a total of about 4,500 people, those who took
Contrave lost an average of 4.2 percentage points of their weight more than
those getting a placebo. This is below the F.D.A. standard of 5 percent.
However, the drug did meet a second requirement that twice as many patients on
the drug as on the placebo lose at least 5 percent of their weight. Meeting only
one of the two criteria is enough for approval.
There were also concerns that the drug could cause seizures and psychiatric or
cognitive problems.
The F.D.A.’s decision is also a setback for Takeda Pharmaceutical of Japan,
which had acquired the American marketing rights from Orexigen. It is also
possible that Takeda might withdraw from the partnership, Orexigen executives
said during a conference call.
F.D.A. Declines to
Approve Diet Drug, NYT, 1.2.2011,
http://www.nytimes.com/2011/02/02/business/02drug.html
Federal
Judge Rules That Health Law Violates Constitution
January 31,
2011
The New York Times
By KEVIN SACK
A second
federal judge ruled on Monday that it was unconstitutional for Congress to enact
a health care law that required Americans to obtain commercial insurance,
evening the score at 2 to 2 in the lower courts as conflicting opinions begin
their path to the Supreme Court.
But unlike a Virginia judge in December, Judge Roger Vinson of Federal District
Court in Pensacola, Fla., concluded that the insurance requirement was so
“inextricably bound” to other provisions of the Affordable Care Act that its
unconstitutionality required the invalidation of the entire law.
“The act, like a defectively designed watch, needs to be redesigned and
reconstructed by the watchmaker,” Judge Vinson wrote.
The judge declined to immediately enjoin, or suspend, the law pending appeals, a
process that could last two years. But he wrote that the federal government
should adhere to his declaratory judgment as the functional equivalent of an
injunction. That left confusion about how the ruling might be interpreted in the
26 states that are parties to the legal challenge.
The insurance mandate does not take effect until 2014. But many new regulations
are already operating, like requirements that insurers cover children with
pre-existing health conditions and eliminate lifetime caps on benefits. States
are also preparing for a major expansion of Medicaid eligibility and the
introduction of health insurance exchanges in 2014.
David B. Rivkin Jr., a lawyer for the states, said the ruling relieved the
plaintiff states of any obligation to comply with the health law. “With regard
to all parties to this lawsuit, the statute is dead,” Mr. Rivkin said.
But White House officials declared that the opinion should not deter the
continuing rollout of the law. “Implementation would continue apace,” a senior
administration official said. “This is not the last word by any means.”
At the same time, Stephanie Cutter, an assistant to the president, noted in a
post on the White House blog that the ruling had struck down the entire law. She
called it “a plain case of judicial overreaching,” and added, “The judge’s
decision puts all of the new benefits, cost savings and patient protections that
were included in the law at risk.”
The Justice Department, which represents the Obama administration in the
litigation, said it was exploring options to clarify the uncertainty, including
requesting a stay of the decision, either from Judge Vinson or from the United
States Court of Appeals for the Eleventh Circuit.
On Capitol Hill, Republicans sent out a stream of e-mails praising the ruling,
while Senator Richard J. Durbin, Democrat of Illinois, said he would convene a
Judiciary Committee hearing on Wednesday to examine the constitutionality of the
law.
In his 78-page opinion, Judge Vinson held that the insurance requirement
exceeded the regulatory powers granted to Congress under the Commerce Clause of
the Constitution. He wrote that the provision could not be rescued by an
associated clause in Article I that gives Congress broad authority to make laws
“necessary and proper” to carrying out its designated responsibilities.
“If Congress can penalize a passive individual for failing to engage in
commerce, the enumeration of powers in the Constitution would have been in
vain,” the judge asserted.
In a silver lining for the Obama administration, Judge Vinson rejected a second
claim that the new law violated state sovereignty by requiring states to pay for
a fractional share of the planned Medicaid expansion.
The judge’s ruling came in the most prominent of more than 20 legal challenges
to the sweeping health law, which was signed last March by President Obama.
The plaintiffs include governors and attorneys general from 26 states, all but
one of them Republicans, as well as the National Federation of Independent
Business, which represents small companies. Officials from six states joined the
lawsuit in January after shifts in party control brought by November’s
elections.
The ruling by Judge Vinson, a senior judge who was appointed by President Ronald
Reagan, solidified the divide in the health litigation among judges named by
Republicans and those named by Democrats.
In December, Judge Henry E. Hudson of Federal District Court in Richmond, Va.,
who was appointed by President George W. Bush, became the first to invalidate
the insurance mandate. Two other federal judges named by President Bill Clinton,
a Democrat, have upheld the law.
Judge Vinson’s opinion hangs on a series of Supreme Court decisions that have
defined the limits of the Commerce Clause by granting Congress authority to
regulate “activities that substantially affect interstate commerce.”
The plaintiffs characterized the insurance requirement as an unprecedented
effort to regulate inactivity because citizens would be assessed an income tax
penalty for failing to buy a product.
Justice Department lawyers responded that a choice not to obtain health
insurance was itself an active decision that, taken in the aggregate, shifted
the cost of caring for the uninsured to hospitals, governments and privately
insured individuals.
In his decision, Judge Vinson wrote, “It would be a radical departure from
existing case law to hold that Congress can regulate inactivity under the
Commerce Clause.” If Congress has such power, he continued, “it is not
hyperbolizing to suggest that Congress could do almost anything it wanted.”
The Pensacola case is now likely to head to the Eleventh Circuit in Atlanta,
considered one of the country’s most conservative appellate benches. The
Richmond case is already with another conservative court, the United States
Court of Appeals for the Fourth Circuit in Richmond, which has set oral
arguments for May.
That court will consider diametrically opposed rulings from courthouses situated
116 miles apart, as it was a judge in Lynchburg, Va., Norman K. Moon, who issued
one of the two decisions upholding the law. Meanwhile, the United States Court
of Appeals for the Sixth Circuit in Cincinnati is already receiving briefs on
the other decision backing the law, which was delivered by Judge George C. Steeh
in Detroit.
Judge Vinson’s ruling further arms Republicans in Congress who are waging a
fierce campaign against the health care act. The new Republican majority in the
House voted this year to repeal the law, a largely symbolic measure that is
given no chance in the Democratic-controlled Senate.
The Obama administration argues that without the insurance mandate consumers
might simply wait until they are sick to enroll, undercutting the actuarial
soundness of risk pooling and leading to an industry “death spiral.”
But the mandate’s legal and political problems have prompted a few Democratic
senators to join Republicans in exploring alternatives that would encourage
citizens to buy insurance without requiring it.
For instance, people could be given a narrow window to enroll, and those who
miss the deadline would face lengthy waiting periods for coverage.
Alternately, those who apply late and are eligible for government tax credits
under the law coverage could be penalized through a reduction of their
subsidies.
Sheryl Gay Stolberg contributed reporting.
Federal Judge Rules That Health Law Violates Constitution,
NYT, 31.1.2011,
http://www.nytimes.com/2011/02/01/us/01ruling.html
The Two Abortion Wars: State Battles Over Roe v. Wade
January 29, 2011
The New York Times
Away from Washington, another ominous anti-abortion battle is accelerating in
the states. Anti-abortion forces have been trying to take advantage of the 2007
ruling in which the Supreme Court upheld a federal ban on a particular method of
abortion.
In 2010, more than 600 measures were introduced in state legislatures to limit
access to abortion and some 34 secured passage, according to tallies by Naral
Pro-Choice America and the Center for Reproductive Rights. November’s elections
made the outlook even bleaker.
Twenty-nine governors are considered solidly anti-abortion, up from 21 before
the election. In 15 states, both the legislature and the governor are
anti-abortion, compared with 10 last year. This math greatly increases the
prospect of extreme efforts to undermine abortion access with Big Brother
measures that require physicians to read scripts about fetal development and
provide ultrasound images, and that impose mandatory waiting periods or create
other unnecessary regulations.
Such restrictions, combined with a persistent atmosphere of intimidation and
violence, have taken a grievous toll on the fundamental right protected by Roe
v. Wade, the 1973 decision that recognized a woman’s constitutional right to
make her own child-bearing decisions. Eighty-seven percent of counties have no
abortion provider, according to the Guttmacher Institute.
For the moment, most state legislatures are preoccupied with budget crises, so
the next abortion battles are still taking shape. However, there are at least
two areas where anti-abortion forces will be active in 2011.
The first is the fight over health insurance. The second is the expanding effort
to ban later abortions.
Reigning Supreme Court precedent restricts the government’s ability to bar
abortions prior to the point considered to be the earliest a fetus could survive
outside the womb, around 22 to 26 weeks after conception.
Nebraska enacted a law last year directly challenging the viability standard.
The statute, which went into effect in October, bans abortions 20 weeks after
conception. It includes a very narrow exception for a woman’s life and physical
health, and lacks any exception for the discovery of severe fetal anomalies.
Copycat laws are now pending in other states.
About 90 percent of abortions take place in the first trimester, but that does
not excuse some states’ efforts to require women to continue pregnancies after a
tragic fetal diagnosis or pregnancies that result from rape or incest. The
objective is to provide the Supreme Court’s conservative majority with a new
vehicle for further tampering with Roe v. Wade’s insight that the decision about
whether to terminate a pregnancy is best left to women and their doctors
pre-viability.
Americans who support women’s reproductive rights and oppose this kind of
outrageous government intrusion need to respond with rising force and clarity to
this real and immediate danger.
The Two Abortion Wars:
State Battles Over Roe v. Wade, NYT, 29.1.2011,
http://www.nytimes.com/2011/01/30/opinion/30sun2.html
Do Emotions Play a Role in Illness?
January 29, 2011
The New York Times
To the Editor:
Re “A Fighting Spirit Won’t
Save Your Life,” by Richard P. Sloan (Op-Ed, Jan. 25):
Dr. Sloan cites a Finnish study to support his belief that emotions have no role
in disease. In fact, this study examined extroversion and neuroticism as risk
factors for cancer, not “a fighting spirit” or other positive emotions.
A wide body of evidence has shown clearly that our emotions often play a role in
illness. Chronic anger, hostility and depression significantly increase the risk
of coronary heart disease. Chronic emotional stress shortens telomeres, the ends
of our chromosomes that control how long we live. Support groups prolong
survival in women with metastatic breast cancer.
To empower is not to blame. It’s not all in our genes — for example, meditation
beneficially changes gene expression. Positive emotions don’t always override
our genes, but they can play an important role. We’re not victims; our genes are
a predisposition, but our genes are not our fate.
Dean Ornish
Sausalito, Calif., Jan. 25, 2011
The writer is founder and president of the Preventive Medicine Research
Institute and a clinical professor of medicine at the University of California,
San Francisco.
•
To the Editor:
Dr. Richard P. Sloan is quite justified in puncturing the myth that one’s
character or attitude greatly affects the development or outcome of serious
illness. But as Dr. Sloan knows, the story becomes more complex when clinically
significant depression accompanies certain other medical conditions.
For example, there is probably a “bidirectional relationship” between coronary
artery disease and major depression. A recent review by Dr. I. S. Khawaja and
colleagues concluded that coronary artery disease can cause depression, and that
depression is an independent risk factor for coronary artery disease and its
complications.
Although the evidence is not conclusive, some data suggest that appropriate
treatment of the accompanying depression may decrease cardiovascular risk
factors as well. Finally, a “positive attitude” can and often does play a role
in enhancing rehabilitation and adherence to medication, in a variety of
diseases.
Ronald Pies
Lexington, Mass., Jan. 25, 2011
The writer is a psychiatrist associated with SUNY Upstate Medical University and
Tufts University School of Medicine.
•
To the Editor:
Having lost someone to cancer, someone who loved life and lived it more fully
than most of us, I give my appreciation to Richard P. Sloan for his article
citing studies showing “no significant association between personality traits
and the likelihood of developing or surviving cancer.”
If a fighting spirit were key to conquering cancer, then we might want to send
patients to psychotherapy rather than to a clinical trial. Perhaps it would
distract us from the return on the dollar that has been invested in cancer
research so far.
Perhaps it would deaden the connotation that if those who survive a potentially
fatal disease are fighters, then those who succumb are not. They are losers.
We all know that this is not true. We see terrifically brave and stoic people
die each day from a disease of the body that has not daunted their spirit.
Please, let’s drop the battleground lexicon and treat all those dealing with
such serious disease with more compassion and understanding.
Melissa Cole
Elgin, Tex., Jan. 25, 2011
•
To the Editor:
Richard P. Sloan argues that “positive characteristics like optimism,
spirituality and being a compassionate person” have no enhancing effects on
health and longevity. Although we endorse his skepticism regarding scientific
evidence for the power of positive thinking, it is critical to qualify his
point, so as not to throw the baby out with the bath water.
For example, our work, and that of others, has demonstrated that helping
behavior (and accompanying compassionate motives) are associated with reduced
morbidity and mortality for the helper. We are exploring the physiological basis
for compassionate motivation, and how that physiology is related to stress, and
the extent to which it mitigates the effects of disease.
Given the well-documented relationship between stress and immune system
functioning, we must not let misinterpretation and misrepresentation of some
scientific findings obscure others, or delay discoveries that might save lives.
Stephanie L. Brown
R. Michael Brown
Stony Brook, N.Y., Jan. 25, 2011
The writers are, respectively, an associate professor of preventive medicine at
Stony Brook University and professor emeritus of psychology at Pacific Lutheran
University.
•
To the Editor:
Richard P. Sloan’s rational and compassionate analysis of the scientific
evidence is a boon to all who live with illness and feel that they are somehow
to blame if they do not recover.
While it is true that optimism and positive thinking cannot overcome illness, it
is also true that religious hope and trust in God do not ensure recovery. Belief
in a loving God is a source of comfort and strength for millions of people when
they are faced with illness. Yet just as “the rain falls on the just and the
unjust,” so, too, illness comes to the believer and the unbeliever alike.
None of the great religions of the world promise protection from the
vicissitudes of life. Instead, they teach us to care for one another when
trouble strikes.
In my ministry I have counseled hundreds of people who are racked with guilt
because they feel that their faith was not strong enough to bring healing. Pray
for strength and healing, yes, but recognize that not everything that happens is
God’s will. To borrow a phrase, linking health to personal faith is not only bad
science, it’s also bad religion.
(Rev.) David W. Spollett
Fairfield, Conn., Jan. 26, 2011
•
To the Editor:
A fighting spirit alone may not save your life, as Dr. Richard P. Sloan argues.
But it can get you a lot more attention, especially in today’s understaffed
health care facilities. And that attention can save your life.
Patrick Maney
Chestnut Hill, Mass., Jan. 25, 2011
Do Emotions Play a Role
in Illness?, NYT, 29.1.2011,
http://www.nytimes.com/2011/01/30/opinion/l30health.html
A Fighting Spirit Won’t Save Your Life
January 24, 2011
The New York Times
By RICHARD P. SLOAN
GABRIELLE GIFFORDS’S remarkable recovery from a bullet to her head has
provided a heartening respite from a national calamity. Representative
Giffords’s husband describes her as a “fighter,” and no doubt she is one.
Whether her recovery has anything to do with a fighting spirit, however, is
another matter entirely.
The idea that an individual has power over his health has a long history in
American popular culture. The “mind cure” movements of the 1800s were based on
the premise that we can control our well-being. In the middle of that century,
Phineas Quimby, a philosopher and healer, popularized the view that illness was
the product of mistaken beliefs, that it was possible to cure yourself by
correcting your thoughts. Fifty years later, the New Thought movement, which the
psychologist and philosopher William James called “the religion of the healthy
minded,” expressed a very similar view: by focusing on positive thoughts and
avoiding negative ones, people could banish illness.
The idea that people can control their own health has persisted through Norman
Vincent Peale’s “Power of Positive Thinking,” in 1952, to a popular book today,
“The Secret,” by Rhonda Byrne, which teaches that to achieve good health all we
have to do is to direct our requests to the universe.
It’s true that in some respects we do have control over our health. By
exercising, eating nutritious foods and not smoking, we reduce our risk of heart
disease and cancer. But the belief that a fighting spirit helps us to recover
from injury or illness goes beyond healthful behavior. It reflects the
persistent view that personality or a way of thinking can raise or reduce the
likelihood of illness.
The psychosomatic hypothesis, which was popular in the mid-20th century, held
that repressed emotional conflict was at the core of many physical diseases:
Hypertension was the product of the inability to deal with hostile impulses.
Ulcers were caused by unresolved fear and resentment. And women with breast
cancer were characterized as being sexually inhibited, masochistic and unable to
deal with anger.
Although modern doctors have rejected those beliefs, in the past 20 years, the
medical literature has increasingly included studies examining the possibility
that positive characteristics like optimism, spirituality and being a
compassionate person are associated with good health. And books on the health
benefits of happiness and positive outlook continue to be best sellers.
But there’s no evidence to back up the idea that an upbeat attitude can prevent
any illness or help someone recover from one more readily. On the contrary, a
recently completed study of nearly 60,000 people in Finland and Sweden who were
followed for almost 30 years found no significant association between
personality traits and the likelihood of developing or surviving cancer. Cancer
doesn’t care if we’re good or bad, virtuous or vicious, compassionate or
inconsiderate. Neither does heart disease or AIDS or any other illness or
injury.
And while we may be able to point anecdotally to a Gabrielle Giffords as an
example of how a fighting spirit improves medical outcome, other people with a
spirit just as strong die — think of Elizabeth Edwards, for example. And many
patients who employ negative thinking nevertheless recover from illness every
day. We want good things to happen to good people and this desire blinds us to
evidence to the contrary.
But such beliefs have implications for how we regard people who are ill. If
people are insufficiently upbeat after a cancer diagnosis or inadequately
“spiritual” after a diagnosis of AIDS, are we to assume they have willfully
placed their health at risk? And if they fail to recover, is it really their
fault? The incessant pressure to be positive imposes an enormous burden on
patients whose course of treatment doesn’t go as planned.
Very early in my career, I participated in a study of young women who were
hospitalized and awaiting the results of biopsies to determine if they had
cervical cancer. While I was interviewing one of my patients, the biopsy results
of the woman in the next bed came back to her — negative. The fortunate woman’s
father, who was there with her, said in relief: “We’re good people. We deserve
this.” It was a perfectly understandable response, but what should my patient
have said to herself when her biopsy came back positive? That she got cancer
because she wasn’t a good person?
It is difficult enough to be injured or gravely ill. To add to this the burden
of guilt over a supposed failure to have the right attitude toward one’s illness
is unconscionable. Linking health to personal virtue and vice not only is bad
science, it’s bad medicine.
Richard P. Sloan, a professor of behavioral medicine at Columbia University
Medical Center, is the author of “Blind Faith.”
A Fighting Spirit Won’t Save Your Life, NYT, 24.1.2011,
http://www.nytimes.com/2011/01/25/opinion/25sloan.html
What Comes After No?
January 24, 2011
The New York Times
The Republicans have vowed to “repeal and replace” President
Obama’s historic health care reform law. Now that House Republicans have muscled
through a symbolic repeal bill, they will have to deliver their own alternative
plan. Don’t expect much.
There are many more slogans than details. But it is already clear that their
approach would do almost nothing to control skyrocketing health care costs and
would provide little help to the 50 million uninsured Americans.
When Republican leaders talk of reducing medical costs they really mean reducing
insurance premiums for some people, primarily by letting the young and healthy
buy insurance in states that allow the sale of skimpy policies. That won’t help
older and less healthy people and would probably drive up their premiums as they
flock to states whose regulations guarantee them coverage.
The Republicans have offered no coherent plan for slowing the rapid rise in
medical costs that is driving up insurance premiums, Medicare and Medicaid
costs, and the federal deficit. The reform law, by contrast, has multiple
provisions for changing the delivery of health care in ways that should reduce
costs.
As for the Republicans’ calls to reduce waste and fraud in Medicare, reform the
medical malpractice system, and expand high-risk pools to cover people with
pre-existing conditions, most of these ideas are already in the reform law. They
could surely be strengthened if both parties worked together.
Even as it denounces reform at every turn, the Republican leadership has figured
out that many Americans want the many consumer protections that come with the
new law. So, once reform is repealed, the leaders are vowing to reinstate such
provisions as letting young people stay on their parents’ plans until age 26,
preventing insurers from canceling policies after people become sick, and
barring insurers from placing caps on what they will pay.
The problem is that such requirements will drive up the cost of insurance unless
they are paired with a mandate (or comparable prod) requiring that everyone buy
insurance so that healthy people offset the costs of less healthy beneficiaries.
Yes, that’s the same mandate the Republicans have vowed to overturn.
Many Republicans have also vowed to restore more than $130 billion worth of
unjustified subsidies to private Medicare Advantage plans that is needed to help
pay for the expansion of coverage under health care reform.
In coming weeks, expect to see a lot more posturing on issues that might
energize the party’s conservative base or poll well with people made skittish by
months of Republican exaggerations about the new reform law. They have already
introduced bills making it even harder for insurance policies in new insurance
exchanges to cover abortions, never mind that the law already has incredibly
strict provisions.
The Party of No will also try to use its new control of the House to block
implementation of reform by withholding money needed to hire people to write
necessary regulations. The House Republican Study Committee has proposed
legislation that would prohibit using money in the annual budget to carry out
any provision of the law or to defend it in court.
The Republicans need to explain how they plan to address the problems of
covering the uninsured, wrestling down medical costs and controlling the
deficit. Just saying no isn’t enough.
What Comes After No?, NYT,
24.1.2011,
http://www.nytimes.com/2011/01/25/opinion/25tue1.html
Lawmakers in Many States Pushing for Abortion Curbs
January 21, 2011
The New York Times
By ERIK ECKHOLM
Newly energized by their success in November’s midterm elections,
conservative legislators in dozens of states are mounting aggressive campaigns
to limit abortions.
The lawmakers are drafting, and some have already introduced, bills that would
ban most abortions at 20 weeks after conception, push women considering
abortions to view a live ultrasound of the fetus, or curb insurance coverage,
among other proposals.
In Florida and Kansas, legislators plan to reintroduce measures that were vetoed
by previous governors but have the support of the new chief executives, like
ultrasound requirements and more stringent regulation of late-term abortions.
“I call on the Legislature to bring to my desk legislation that protects the
unborn, establishing a culture of life in Kansas,” Gov. Sam Brownback said last
week in his first State of the State message.
“This is the best climate for passing pro-life laws in years,” said Michael
Gonidakis, executive director of Ohio Right to Life, expressing the mood in many
states. “We’ve got a pro-life governor and a brand new pro-life speaker. Our
government now is pro-life from top to bottom.”
Abortion opponents plan marches in Washington and elsewhere this weekend and on
Monday to mark the anniversary of the 1973 Supreme Court decision, Roe v. Wade,
that established a woman’s right to an abortion.
Republicans in Congress hope to strengthen measures to prevent even indirect
public financing of abortions, but laws in the states have the greatest impact
on access to them. Abortion opponents have been emboldened by major changes in
the political landscape, with conservative Republicans making large gains.
Although social issues were often played down in the campaigns, many of the
newly elected governors and legislators are also solidly anti-abortion, causing
advocates of abortion rights to brace for a year of even tougher battles than
usual.
The biggest shift is in the state capitols, with 29 governors now considered to
be solidly anti-abortion, compared with 21 last year. “This is worrisome because
the governors have been the firewall, they’ve vetoed a lot of bad anti-choice
legislation,” said Ted Miller, a spokesman for Naral Pro-Choice America.
In 15 states, compared with 10 last year, both the legislature and the governor
are anti-abortion, according to a new report by Naral, and those joining this
category include larger states like Michigan, Ohio and Wisconsin, as well as
Georgia and Oklahoma. Maine and Pennsylvania are now strongly anti-abortion as
well, if not quite as solidly.
Just which measures will pass is impossible to predict, particularly because
many states are bogged down by budget crises.
Elizabeth Nash, who tracks state policies on abortion for the Guttmacher
Institute, a research organization, said that while states would be preoccupied
with budget issues, it appeared rather likely that more measures would pass this
year than in 2010, which anti-abortion advocates considered a banner year, with
more than 30 restrictive laws adopted in at least nine states.
The elections brought even more gains for their side than expected, said Mary
Spaulding Balch, state policy director of the National Right to Life Committee,
leading her group to call in its affiliates for a special strategy session on
Dec. 7.
While many anti-abortion measures have been adopted or debated over the years,
including requiring parental consent for minors and waiting periods, advocates
have set a few top priorities for the months ahead:
¶Banning abortions earlier in pregnancy. Most states place restrictions on later
abortions, often defined as after fetal viability, or around 22 to 26 weeks
after conception. But last year, Nebraska set what many advocates consider a new
gold standard, banning abortions, unless there is imminent danger to the woman’s
life or physical health, at 20 weeks after conception, on a disputed theory that
the fetus can feel pain at that point. The measure has not been tested in court,
but similar measures pushing back the permissible timing are being developed in
Indiana, Iowa, New Hampshire, Oklahoma and other states.
The 20-week law in Nebraska, which took effect in October, forced a prominent
doctor who performed late-term abortions to leave the state. Jill June,
president of Planned Parenthood of the Heartland, said women suffering from
complicated pregnancies but are not yet sick enough to qualify for an emergency
abortion would be forced to travel to other states. Or, she said, doctors
fearing prosecution will wait until such women become dangerously ill before
considering an abortion.
¶Pressing women to view ultrasounds. While several states encourage women
seeking abortions to view an ultrasound, Oklahoma last year adopted a
requirement that doctors or technicians perform the procedure with the screen
visible to the woman, and explain in detail what she is seeing. The measure is
under court challenge, but the Kentucky Senate has passed a similar bill, and
variants are expected to come up in states including Indiana, Maryland, Montana,
Ohio, Texas, Virginia and Wyoming.
In Florida, former Gov. Charlie Crist vetoed an ultrasound bill. The new
governor, Rick Scott, attacked him for that veto and is expected to support a
new proposal.
¶Banning any abortion coverage by insurance companies in the new health
insurance exchanges. Numerous states are poised to impose the ban on plans that
will be offered to small businesses and individual insurance buyers under the
Obama administration health plan.
The shifts to conservative governors, in particular, have opened new
opportunities for abortion opponents. In Kansas, legislators said they would act
quickly to adopt measures that were previously vetoed, including regulations
that will make it harder to open abortion clinics or to perform abortions in the
second trimester.
“There’s pent-up demand in the Legislature for these changes,” said State
Representative Lance Kinzer, the chairman of the Judiciary Committee in the
Kansas House. Once these long-debated steps are taken, he said, the Legislature
will consider more sweeping restrictions, including banning most abortions after
the 20th week.
The politics of abortion have changed profoundly in some larger states including
Michigan, Pennsylvania and Wisconsin.
“We’re facing the biggest threat to reproductive rights we’ve ever faced in this
state,” said Lisa Subeck, executive director for Naral Pro-Choice Wisconsin.
In Michigan, because of the switch to an anti-abortion governor, “the dominos
are lined up well for us this time,” said Ed Rivet, legislative director for
Right to Life of Michigan. For starters, advocates hope to pass a state ban on
the procedure opponents call partial-birth abortion that had been vetoed twice.
After that, he said, “We have quite a list.”
Many defenders of abortion rights argue that because the election hinged largely
on the economy and the role of government, officials did not receive a mandate
for sweeping new social measures. “This last election was not about these issues
at all,” said Cecile Richards, president of the Planned Parenthood Federation of
America. “We now are concerned about a real overreaching by some state
legislators and governors that will make it very difficult for women to access
reproductive health care.”
Daniel S. McConchie, vice president for government affairs with Americans United
for Life, responded that laws restricting abortion have been adopted right along
by the states and that while he expected large gains in the year ahead, they
will be part of steady trend.
The abortion rate in the United States, which had declined steadily since a 1981
peak of more than 29 abortions per 1,000 women, stalled between 2005 and 2008,
at slightly under 20 abortions per 1,000 women, according to a new report from
the Guttmacher Institute.
Robbie Brown contributed reporting from Atlanta, Dan Frosch from Denver and
Emma Graves Fitzsimmons from Chicago.
Lawmakers in Many States
Pushing for Abortion Curbs, NYT, 21.1.2011,
http://www.nytimes.com/2011/01/22/us/politics/22abortion.html
Why Parents Fear the Needle
January 20, 2011
The New York Times
By MICHAEL WILLRICH
Wellesley, Mass.
DESPITE overwhelming evidence to the contrary, roughly one in five Americans
believes that vaccines cause autism — a disturbing fact that will probably hold
true even after the publication this month, in a British medical journal, of a
report thoroughly debunking the 1998 paper that began the vaccine-autism scare.
That’s because the public’s underlying fear of vaccines goes much deeper than a
single paper. Until officials realize that, and learn how to counter such
deep-seated concerns, the paranoia — and the public-health risk it poses — will
remain.
The evidence against the original article and its author, a British medical
researcher named Andrew Wakefield, is damning. Among other things, he is said to
have received payment for his research from a lawyer involved in a suit against
a vaccine manufacturer; in response, Britain’s General Medical Council struck
him from the medical register last May. As the journal’s editor put it, the
assertion that the measles-mumps-rubella vaccine caused autism “was based not on
bad science but on a deliberate fraud.”
But public fear of vaccines did not originate with Dr. Wakefield’s paper.
Rather, his claims tapped into a reservoir of doubt and resentment toward this
life-saving, but never risk-free, technology.
Vaccines have had to fight against public skepticism from the beginning. In
1802, after Edward Jenner published his first results claiming that scratching
cowpox pus into the arms of healthy children could protect them against
smallpox, a political cartoon appeared showing newly vaccinated people with
hooves and horns.
Nevertheless, during the 19th century vaccines became central to public-health
efforts in England, Europe and the Americas, and several countries began to
require vaccinations.
Such a move didn’t sit comfortably with many people, who saw mandatory
vaccinations as an invasion of their personal liberty. An antivaccine movement
began to build and, though vilified by the mainstream medical profession, soon
boasted a substantial popular base and several prominent supporters, including
Frederick Douglass, Leo Tolstoy and George Bernard Shaw, who called vaccinations
“a peculiarly filthy piece of witchcraft.”
In America, popular opposition peaked during the smallpox epidemic at the turn
of the 20th century. Health officials ordered vaccinations in public schools, in
factories and on the nation’s railroads; club-wielding New York City policemen
enforced vaccinations in crowded immigrant tenements, while Texas Rangers and
the United States Cavalry provided muscle for vaccinators along the Mexican
border.
Public resistance was immediate, from riots and school strikes to lobbying and a
groundswell of litigation that eventually reached the Supreme Court. Newspapers,
notably this one, dismissed antivaccinationists as “benighted and deranged” and
“hopeless cranks.”
But the opposition reflected complex attitudes toward medicine and the
government. Many African-Americans, long neglected or mistreated by the white
medical profession, doubted the vaccinators’ motives. Christian Scientists
protested the laws as an assault on religious liberty. And workers feared, with
good reason, that vaccines would inflame their arms and cost them several days’
wages.
Understandably, advocates for universal immunization then and now have tended to
see only the harm done by their critics. But in retrospect, such wariness was
justified: at the time, health officials ordered vaccinations without ensuring
the vaccines were safe and effective.
Public confidence in vaccines collapsed in the fall of 1901 when newspapers
linked the deaths of nine schoolchildren in Camden, N.J., to a commercial
vaccine allegedly tainted with tetanus. In St. Louis, 13 more schoolchildren
died of tetanus after treatment with the diphtheria antitoxin. It was decades
before many Americans were willing to submit to public vaccination campaigns
again.
Nevertheless, the vaccination controversy of the last century did leave a
positive legacy. Seeking to restore confidence after the deaths in Camden and
St. Louis, Congress enacted the Biologics Control Act of 1902, establishing the
first federal regulation of the nation’s growing vaccine industry. Confronted
with numerous antivaccination lawsuits, state and federal courts established new
standards that balanced public health and civil liberties.
Most important, popular resistance taught government officials that when it
comes to public health, education can be more effective than brute force. By
midcentury, awareness efforts had proven critical to the polio and smallpox
vaccination efforts, both of which were huge successes.
One would think such education efforts would no longer be necessary. After all,
today’s vaccines are safer, subject to extensive regulatory controls. And shots
are far more numerous: as of 2010, the Centers for Disease Control recommended
that every child receive 10 different vaccinations. For most Americans, vaccines
are a fact of life.
Still, according to a 2010 C.D.C. report, 40 percent of American parents with
young children have delayed or refused one or more vaccines for their child.
That’s in part because vaccines have been so successful that any risk associated
with their use, however statistically small, takes on an elevated significance.
It also doesn’t help that, thanks to the Internet, a bottomless archive of
misinformation, including Dr. Wakefield’s debunked work, is just a few
keystrokes away. All of which means the public health community must work even
harder to spread the positive news about vaccines.
Health officials often get frustrated with public misconceptions about vaccines;
at the turn of the last century, one frustrated Kentucky health officer pined
for the arrival of “the fool-killer” — an outbreak of smallpox devastating
enough to convince his skeptical rural constituency of the value of vaccination.
But that’s no way to run a health system. Our public health leaders would do far
better to adopt the strategy used by one forward-thinking federal health
official from the early 20th century, C. P. Wertenbaker of the Public Health and
Marine-Hospital Service.
As smallpox raged across the American South, Wertenbaker journeyed to small
communities and delivered speech after speech on vaccinations before swelling
audiences of townsfolk, farmers and families. He listened and replied to
people’s fears. He told them about the horrors of smallpox. He candidly
presented the latest scientific information about the benefits and risks of
vaccination. And he urged his audiences to protect themselves and one another by
taking the vaccine. By the time he was done, many of his listeners were already
rolling up their sleeves.
America’s public health leaders need to do the same, to reclaim the town square
with a candid national conversation about the real risks of vaccines, which are
minuscule compared with their benefits. Why waste another breath vilifying the
antivaccination minority when steps can be taken to expand the pro-vaccine
majority?
Obstetricians, midwives and pediatricians should present the facts about
vaccines and the nasty diseases they prevent early and often to expectant
parents. Health agencies should mobilize local parents’ organizations to
publicize, in realistic terms, the hazards that unvaccinated children can pose
to everyone else in their communities. And health officials must redouble their
efforts to harness the power of the Internet and spread the good word about
vaccines.
You can bet that Wertenbaker would have done the same thing.
Michael Willrich, an associate professor of history at Brandeis University, is
the author of the forthcoming “Pox: An American History.”
Why Parents Fear the
Needle, NYT, 20.1.2011,
http://www.nytimes.com/2011/01/21/opinion/21willrich.html
House
Votes for Repeal of Health Law in Symbolic Act
January 19,
2011
By THE NEW YORK TIMES
By DAVID M. HERSZENHORN and ROBERT PEAR
WASHINGTON
— The House voted Wednesday to repeal the Democrats’ landmark health care
overhaul, marking what the new Republican majority in the chamber hailed as the
fulfillment of a campaign promise and the start of an all-out effort to
dismantle President Obama’s signature domestic policy achievement.
The vote was 245 to 189, with 3 Democrats joining all 242 Republicans in support
of the repeal.
Leaders of the Democratic-controlled Senate have said that they will not act on
the repeal measure, effectively scuttling it.
While conceding that reality, House Republicans said they would press ahead with
their “repeal and replace” strategy. But the next steps will be much more
difficult, as they try to forge consensus on alternatives emphasizing “free
market solutions” to control health costs and expand coverage.
Even as four House committees begin drafting legislation, Republicans said they
would seek other ways to stop the overhaul, by choking off money needed to carry
it out and by pursuing legislation to undo specific provisions, like a
requirement for most Americans to carry health insurance or face penalties. The
law is also under challenge in the federal courts, with the individual coverage
requirements fueling a constitutional battle likely to be decided by the Supreme
Court.
The House vote was the first stage of a Republican plan to use the party’s
momentum coming out of the midterm elections to keep the White House on the
defensive, and will be followed by a push to scale back federal spending. In
response, the administration struck a more aggressive posture than it had during
the campaign to sell the health care law to the public. With many House
Democrats from swing districts having lost their seats in November, the
remaining Democrats held overwhelmingly together in opposition to the repeal.
On the House floor, the resulting debate was a striking reprise of the one that
engulfed Capitol Hill from the spring of 2009 until March 2010, when Mr. Obama
signed the health care law.
And while the tone was slightly subdued in the aftermath of the attempted
assassination of Representative Gabrielle Giffords in Arizona, the debate showed
that the divisions over the law remained as deep as ever.
The three Democrats who crossed the aisle to support the repeal were
Representatives Dan Boren of Oklahoma, Mike McIntyre of North Carolina, and Mike
Ross of Arkansas, all of whom opposed the law last year.
Ms. Giffords, who had supported the law, remains hospitalized in Arizona and was
the only House member who did not vote.
Republicans denounced the law as an intrusion by the government that would
prompt employers to eliminate jobs, create an unsustainable entitlement program,
saddle states and the federal government with unmanageable costs, and interfere
with the doctor-patient relationship. Republicans also said the law would
exacerbate the steep rise in the cost of medical services.
“Repeal means paving the way for better solutions that will lower the cost
without destroying jobs or bankrupting our government,” the House speaker, John
A. Boehner of Ohio, said. “Repeal means keeping a promise. This is what we said
we would do.”
Democrats, eager for a second chance to sell the law, trumpeted the benefits
that have already taken effect. These include protections for people who would
otherwise be denied insurance coverage based on a pre-existing medical
condition, the ability for children to stay on their parents’ policy until age
26, and new tax breaks for small businesses that provide health coverage to
their workers.
Representative John Lewis, Democrat of Georgia, said, “It is unbelievable that
with so many people out of work and millions of people uninsured, the first act
of this new Congress is to take health care away from people who just got
coverage.”
The health care law, which Congress approved last year without a single
Republican in favor, seeks to extend insurance to more than 30 million people by
expanding Medicaid and providing federal subsidies to help lower and
middle-income Americans buy private coverage.
Republican leaders said they had not set any timetable for the four committees
drafting alternatives to the law. “I don’t know that we need artificial
deadlines for the committees to act,” Mr. Boehner said. “We expect them to act
in an efficient way.”
Republicans said their package would probably include proposals to allow sales
of health insurance across state lines; to help small businesses band together
and buy insurance; to limit damages in medical malpractice suits; and to promote
the use of health savings accounts, in combination with high-deductible
insurance policies.
Republicans also want to help states expand insurance pools for people with
serious illnesses. The new law includes such pools, as an interim step until
broader insurance coverage provisions take effect in 2014, but enrollment has
fallen short of expectations.
Representative Paul Broun, Republican of Georgia, said that allowing people to
buy insurance across state lines would “expand choice and competition.” And he
said businesses could negotiate better insurance rates if they could join
together in “association health plans,” sponsored by trade and professional
groups.
But state insurance officials have resisted such proposals, on the ground that
they would weaken state authority to regulate insurance and to enforce consumer
protections -- a concern shared by Congressional Democrats.
Some Republicans seemed sensitive to accusations that repeal would strip away
new patient protections and leave millions of Americans without insurance.
Representative Joe Heck, Republican of Nevada and a physician, said he supported
some goals of the new law: “making sure people don’t lose their coverage once
they get sick; letting dependent children stay on their parents’ insurance until
they turn 26; making sure anyone who wants to buy insurance can purchase a
policy, regardless of pre-existing conditions.”
Representative Joe L. Barton, Republican of Texas, said, “There are some things
in the new law that we think are worth keeping,” including a procedure for
approval of generic versions of expensive biotechnology drugs.
But Mr. Barton and other Republicans returned to a core objection to the law,
which they said extends the reach of government too far.
“We believe that you shouldn’t have the federal government mandate that an
individual has to have health insurance, whether he or she wants it,” Mr. Barton
said. “We want to repeal today so that we can begin to replace tomorrow.”
Representative Allyson Y. Schwartz, Democrat of Pennsylvania, said she doubted
that the Republican alternatives would be effective in expanding coverage or
controlling costs.
“Many Republicans want to repeal the law, but are not serious about replacing
it,” Ms. Schwartz said.
House Votes for Repeal of Health Law in Symbolic Act, NYT,
19.1.2011,
http://www.nytimes.com/2011/01/20/health/policy/20cong.html
Basic Questions, Elusive Answers on Health Law
January 18, 2011
The New York Times
By DAVID M. HERSZENHORN and ROBERT PEAR
WASHINGTON — As the fight over health care returned to the House floor on
Tuesday, the debate could largely be stripped down to four questions that are
relatively simple to ask, if not to answer:
Will the health care law, approved last year by Democrats with no Republican
support, increase or reduce future federal deficits?
Will the law lead to the elimination of jobs by overburdened employers as
Republicans assert, or will it create jobs as Democrats maintain?
Will the law raise or lower the cost of medical care for individuals and
families, employers, and state and federal governments?
And, will the law achieve President Obama’s goal of providing coverage to more
than 30 million uninsured Americans?
Given the complexity of the issues, none of these questions can yet be answered
definitively.
More certain is the fate of the Republicans’ bill to repeal the law, which
contains 24 lines of legislative text and 38 lines of the names of the lawmakers
sponsoring it. While House Republicans will vote to approve it on Wednesday, the
Democratic-controlled Senate is highly unlikely to act on it.
Still, the assertions from the two sides highlight their radically different
views about the proper role of government and market forces in the health care
system. It is a policy fight that is likely to rage for the next two years in
Congress and to figure prominently in the 2012 presidential campaign.
As floor debate on the repeal measure opened on Tuesday, Representative Paul
Ryan, Republican of Wisconsin and chairman of the Budget Committee, who is a
respected voice on fiscal issues, declared that the health care law would
“accelerate our country’s path toward bankruptcy.”
Mr. Ryan expressed one of the Republicans’ main complaints: that Democrats and
independent Congressional budget analysts have underestimated the costs of the
law, which Republicans say will ultimately add hundreds of billions of dollars
to future federal deficits.
The nonpartisan Congressional Budget Office disagrees.
In its official analysis, the budget office estimated that the cost of new
benefits in the health care law would be more than offset by revenues from new
taxes and by cuts in projected Medicare spending, reducing future deficits.
Repealing the law, the budget office has predicted, would add $230 billion to
federal deficits from 2012 to 2021.
Republicans dispute that, saying the cost will be far higher than expected.
“We believe that it is an unsustainable, open-ended entitlement that could very
well bankrupt this country and the states,” the House majority leader,
Representative Eric Cantor, Republican of Virginia, said at a news conference on
Tuesday.
The budget office has said that its estimates are based on the most likely
outcomes, and that the eventual cost of the bill is equally likely to be higher
or lower.
The office has also said that lawmakers may find it difficult to follow through
with some aspects of the law, particularly cuts in projected Medicare spending.
If the cuts do not take hold, the cost of the law could soar.
Democrats, meanwhile, say the law could save even more money than expected
because the budget office does not give them credit for likely improvements in
the delivery of medical services that could slow the growth in costs for
individuals, businesses and the federal and state governments.
Weighing into the debate, Mr. Obama said Tuesday that Americans were already
enjoying many benefits of the new law, and that he would not let Republicans
dismantle it.
“I’m willing and eager to work with both Democrats and Republicans to improve
the Affordable Care Act,” Mr. Obama said in a statement. “But we can’t go
backward.”
The White House and Congressional Democrats said the law would create more than
300,000 jobs, by slowing the growth of health costs so employers would have more
to spend on wages and hiring. In addition, they said, the law provides tax
credits to help many small businesses buy insurance for their employees.
By contrast, Representative Sam Graves, Republican of Missouri and chairman of
the House Committee on Small Business, said the law “could cost our economy 1.6
million jobs, one million of which could come from small businesses.”
Many economists say the effects on jobs are likely to be modest. Most large
companies already provide health benefits to employees. And many small
businesses will be exempt from penalties if they fail to do so.
While employers often pay premiums for their employees, economists say, the cost
of health benefits is, over time, generally passed on to workers, through
reductions in wages or other compensation. But employers cannot reduce the wages
of people earning the minimum wage.
Thus, the Congressional Budget Office says, the new law “will probably cause
some employers to respond by hiring fewer low-wage workers,” or by using more
part-time and seasonal workers.
But Democrats say that if the law provides coverage to more than 30 million
currently uninsured people, as intended, it will increase demand for medical
services, thus creating new job opportunities in the health care industry.
Representative Debbie Wasserman Schultz, Democrat of Florida, said, “There is
not a single area of health care” that will experience job losses as a result of
the law.
Republicans have emphasized the jobs issue, even naming their bill the
“Repealing the Job-Killing Health Care Law Act.” But they have also pressed an
argument that the law does not do much to slow the growth of health spending.
The law includes many provisions intended to restrain medical costs, which have
long grown faster than general inflation.
For example, it would trim Medicare payment rates for hospitals and many other
health care providers; create an independent advisory board to recommend further
savings in Medicare; and encourage doctors and hospitals to coordinate care,
eliminate duplicative tests and reduce the readmission of patients to hospitals.
But experts say they are not sure how effective these provisions will be, and
note that countries around the globe have struggled to control medical costs.
Republicans say the law is geared less to limiting costs than to extending
coverage to the uninsured. The budget office has estimated that by 2019 the law
will have reduced the number of uninsured Americans by 32 million.
But even with a provision in the law requiring that most Americans obtain
insurance, it is possible that the law will not cover as many people as
expected. Some supporters of the law have questioned whether federal subsidies
will be adequate to make insurance affordable for lower- and middle-income
Americans. And while the law includes a broad expansion of Medicaid eligibility,
many people now eligible do not enroll.
In addition, the continuing political controversy around the law has created
even more uncertainty about how people will respond to it.
Basic Questions, Elusive
Answers on Health Law, NYT, 18.1.2011,
http://www.nytimes.com/2011/01/19/us/politics/19cong.html
Getting Someone to Psychiatric Treatment Can Be Difficult and
Inconclusive
January 18, 2011
The New York Times
By A. G. SULZBERGER and BENEDICT CAREY
TUCSON —What are you supposed to do with someone like Jared L. Loughner?
That question is as difficult to answer today as it was in the years and months
and days leading up to the shooting here that left 6 dead and 13 wounded.
Millions of Americans have wondered about a troubled loved one, friend or
co-worker, fearing not so much an act of violence, but — far more likely —
self-inflicted harm, landing in the streets, in jail or on suicide watch. But
those in a position to help often struggle with how to distinguish ominous
behavior from the merely odd, the red flags from the red herrings.
In Mr. Loughner’s case there is no evidence that he ever received a formal
diagnosis of mental illness, let alone treatment. Yet many psychiatrists say
that the warning sings of a descent into psychosis were there for months, and
perhaps far longer.
Moving a person who is resistant into treatment is an emotional, sometimes
exhausting process that in the end may not lead to real changes in behavior.
Mental health resources are scarce in most states, laws make it difficult to
commit an adult involuntarily, and even after receiving treatment, patients
frequently stop taking their medication or seeing a therapist, believing that
they are no longer ill.
The Virginia Tech gunman was committed involuntarily before killing 32 people in
a 2007 rampage.
With Mr. Loughner, dozens of people apparently saw warning signs: the classmates
who listened as his dogmatic language grew more detached from reality. The
police officers who nervously advised that he could not return to college
without a medical note stating that he was not dangerous. His father, who chased
him into the desert hours before the attack as Mr. Loughner carried a black bag
full of ammunition.
“This isn’t an isolated incident,” said Daniel J. Ranieri, president of La
Frontera Center, a nonprofit group that provides mental health services. “There
are lots of people who are operating on the fringes who I would describe as
pretty combustible. And most of them aren’t known to the mental health system.”
Dr. Jack McClellan, an adult and child psychiatrist at the University of
Washington, said he advises people who are worried that someone is struggling
with a mental disorder to watch for three things — a sudden change in
personality, in thought processes, or in daily living. “This is not about
whether someone is acting bizarrely; many people, especially young people,
experiment with all sorts of strange beliefs and counterculture ideas,” Dr.
McLellan said. “We’re talking about a real change. Is this the same person you
knew three months ago?”
Those who have watched the mental unraveling of a loved one say that recognizing
the signs is only the first step in an emotional, often confusing, process.
About half of people with mental illnesses do not receive treatment, experts
estimate, in part because many of them do not recognize that they even have an
illness.
Pushing such a person into treatment is legally difficult in most states,
especially when he or she is an adult — and the attempt itself can shatter the
trust between a troubled soul and the one who is most desperate to help. Others,
though, later express gratitude.
“If the reason is love, don’t worry if they’ll be mad at you,” said Robbie
Alvarez, 28, who received a diagnosis of schizophrenia after being involuntarily
committed when his increasingly erratic behavior led to a suicide attempt. At
the time, he said, he was living in Phoenix with his parents, who he was
convinced were trying to kill him. In Arizona it is easier to obtain an
involuntary commitment than in many states because anyone can request an
evaluation if they observe behavior that suggests a person may present a danger
or is severely disabled (often state laws require some evidence of imminent
danger to self or others).
But there are also questions about whether the system can accommodate an influx
of new patients. Arizona’s mental health system has been badly strained by
recent budget cuts that left those without Medicaid stripped of most of their
services, including counseling and residential treatment, though eligibility
remains for emergency services like involuntary commitment. And the state is
trying to change eligibility requirements for Medicaid, which would potentially
reduce financing further and leave more with limited services.
Still, people who have been through the experience argue that it is better to
act sooner rather than later. “It’s not easy to know when we could or should
intervene but I would rather err on the side of safety than not,” said H. Clarke
Romans, executive director of the local chapter of the National Alliance on
Mental Illness, an advocacy group, who had a son with schizophrenia.
The collective failure to move Mr. Loughner into treatment, either voluntarily
or not, will never be fully understood, because those who knew the young man
presumably wrestled separately and privately about whether to take action. But
the inaction has certainly provoked second-guessing. Sheriff Clarence Dupnik of
Pima County told CNN last Wednesday that Mr. Loughner’s parents were as shocked
as everyone else. “It’s been very, very devastating for them,” he said. “They
had absolutely no way to predict this kind of behavior.”
Linda Rosenberg, president of the National Council for Community Behavioral
Healthcare, said, “The failure here is that we ignored someone for a long time
who was clearly in tremendous distress.” Ms. Rosenberg, whose group is a
nonprofit agency leading a campaign to teach people how to recognize and respond
to signs of mental illness, added, “He wasn’t someone who could ask for help
because his thinking was affected, and as a community no one said, let’s stop
and make sure he gets help.”
At the University of Arizona, where a nursing student killed three instructors
on campus eight years ago before killing himself, feelings of sadness and anger
initially mixed with some guilt as the university examined the missed warning
signs.
The overhauled process for addressing concerns is now more responsive, even if
there are sometimes false alarms, said Melissa M. Vito, vice president for
student affairs. “I guess I’d rather explain why I called someone’s parents than
why I didn’t do something,” she said.
Many others feel the same way.
Four years ago Susan Junck watched her 18-year-old son return from community
college to their Phoenix home one afternoon and, after preparing a snack,
repeatedly call the police to accuse his mother of poisoning him. She assumed it
was an isolated outburst, maybe connected to his marijuana use. In the coming
months, though, her son’s behavior grew more alarming, culminating in an arrest
for assaulting his girlfriend, who was at the center of a number of his
conspiracy theories.
“I knew something was wrong but I literally just did not understand what,” Ms.
Junck, 49, said in a recent interview. “It probably took a year before I
realized my son has a mental illness. This isn’t drug related, this isn’t bad
behavior, this isn’t teenage stuff. This is a serious mental illness.”
Fearful and desperate, she brought her son to an urgent psychiatric center and —
after a five-hour wait — agreed to sign paperwork to have him involuntarily
committed as a danger to himself or others. Her son screamed for her help as he
was carried off. He was diagnosed with paranoid schizophrenia and remains in a
residential treatment facility.
This week Erin Adams Goldman, a suicide prevention specialist with a mental
health nonprofit organization in Tucson, is teaching the first local installment
of a course that is being promoted around the country called mental health first
aid, which instructs participants how to recognize and respond to the signs of
mental illness.
A central tenet is that if a person has suspicions about mental illness it is
better to open the conversation, either by approaching the individual directly,
someone else who knows the person well or by asking for a professional
evaluation.
“There is so much fear and mystery around mental illness that people are not
even aware of how to recognize it and what to do about it,” Ms. Goldman said.
“But we get a feeling when something is not right. And what we teach is to
follow your gut and take some action.”
A. G. Sulzberger reported from Tucson, and Benedict Carey from New York.
Getting Someone to
Psychiatric Treatment Can Be Difficult and Inconclusive, NYT, 18.1.2011,
http://www.nytimes.com/2011/01/19/us/19mental.html
Reproductive Choices Women Face
January 8,
2011
The New York Times
To the Editor:
Re “The Unborn Paradox” (column, Jan. 2):
Ross Douthat seems to be suggesting that women with unintended pregnancies
should bear children rather than have abortions because infertile women want
babies. In doing so, Mr. Douthat ignores the serious health risks that
pregnancies sometimes incur. Should women with unwanted pregnancies be compelled
to take those risks?
Consider New Year’s Eve, a typical night on my obstetrics floor. Several
pregnant women were suffering from complications. Two needed emergency surgery.
One was 19 years old and 20 weeks pregnant with an abnormal fetus. She had
decided to see the pregnancy through. But the amniotic sac ruptured five months
early. We had to stop the heavy bleeding and infection that followed. Her baby
didn’t survive.
Abortion opponents would impose all the risks of pregnancy on women who wish to
end their pregnancies. Instead, let’s make sure that everyone on the
socioeconomic ladder can prevent and plan conception.
Anne Davis
New York, Jan. 3, 2011
The writer, an obstetrician, is medical director of Physicians for Reproductive
Choice and Health.
•
To the Editor:
I have supported abortion rights for as long as I can remember, but nothing
cemented my commitment to women’s reproductive freedom like my own very much
wanted pregnancy nine years ago.
As I grew increasingly delighted about both my experience of pregnancy and
planning for a life with twin babies, I imagined how differently I would feel in
other circumstances. What if I were 14 rather than 34? What if my partner and I
had as many children as we could handle, or more? What if one or both of us were
unemployed?
How might our thrill at the short-term changes in my body and the long-term
changes in our lives transform into dread, depression and anxiety?
Moreover, just because expectant parents are able to think of the fetus as a
baby does not mean it actually is one, and that abortion is the same as the
taking of an actual life, rather than a fantasized one.
Sarah E. Chinn
Brooklyn, Jan. 3, 2011
•
To the Editor:
Ross Douthat provides an eloquent analysis of the abortion conundrum. We embrace
the humanity of our “wanted” babies while we strip the human rights from those
whose conception was unplanned and unwanted. And yet, the circumstances of
conception don’t change the fact that a child in the womb is a separate and
unique human being, morally and ethically entitled to the same rights as you and
I.
Mr. Douthat also points out that adoption has become an unlikely choice for
young mothers like Markai Durham, the subject of an MTV show, who says she
couldn’t bear to give up a child she carried in her womb for nine months, and
opts, instead, to kill that child.
Did anyone along the way point out the deadly flaw in her thinking? Markai and
the million-plus babies who fall into the “unwanted” category every year deserve
to be given a choice that doesn’t involve murder. (Rev.)
Frank Pavone
National Director, Priests for Life
Staten Island, Jan. 3, 2011
•
To the Editor:
What MTV depicted in its documentary “No Easy Decision,” and what Ross Douthat
does not acknowledge in his column, is that Markai Durham and thousands of women
like her are capable of sensitively and wisely weighing the decisions that have
consequences of life or death.
Mr. Douthat offers no evidence that fewer abortions would mitigate complex
fertility treatments or the enormous amount of bureaucratic red tape surrounding
the adoption process. Many studies in fact suggest that, in a culture that
treasures biological children, prospective parents opt first for fertility
treatments and then, if at all, pursue adoption.
A thoughtful look at reproductive decision-making is always welcome, but a
broadside that once again seeks to demonize and make guilty those women who
elect to terminate their pregnancies is not adding to the civil discourse.
Conflating fertility, adoption and abortion in no way alleviates the myriad
challenges involved in deciding whether or not to become a parent.
Joan Malin
President and C.E.O.
Planned Parenthood of New York City
New York, Jan. 3, 2011
•
To the Editor:
I disagree with Ross Douthat’s appraisal of adoption as an answer to unplanned
pregnancies and infertility. I have worked with many pregnant teenagers and
young adult women in my 25 years as a director of an adoption agency, and
adoption is only a small part of the solution.
While I am obviously sympathetic to the desire of infertile couples to become
parents, their needs can never supersede those of pregnant women who are not
prepared to be parents.
Research has shown that abortion very rarely leads to long-term negative
psychological consequences for those women who choose it (myself included).
Yes, of course there is regret and sadness for some women, but carrying a baby
to term and placing him or her for adoption more often than not leads to a
lifetime of pain and sadness, regardless of how right the situation may seem. It
is the right choice for the very few.
Abortion and adoption are two ends of the same spectrum — women having choices
about their reproductive lives. But the agony of a woman placing a child for
adoption cannot be understated.
Randie Bencanann
San Francisco, Jan. 3, 2011
Reproductive Choices Women Face, NYT, 8.1.2011,
http://www.nytimes.com/2011/01/09/opinion/l09douthat.html
The Unborn Paradox
January 2,
2011
The New York Times
By ROSS DOUTHAT
The
American entertainment industry has never been comfortable with the act of
abortion. Film or television characters might consider the procedure, but even
on the most libertine programs (a “Mad Men,” a “Sex and the City”), they’re more
likely to have a change of heart than actually go through with it. Reality TV
thrives on shocking scenes and subjects — extreme pregnancies and surgeries,
suburban polygamists and the gay housewives of New York — but abortion remains a
little too controversial, and a little bit too real.
This omission is often cited as a victory for the pro-life movement, and in some
cases that’s plainly true. (Recent unplanned-pregnancy movies like “Juno” and
“Knocked Up” made abortion seem not only unnecessary but repellent.) But it can
also be a form of cultural denial: a way of reassuring the public that abortion
in America is — in Bill Clinton’s famous phrase — safe and legal, but also rare.
Rare it isn’t: not when one in five pregnancies ends at the abortion clinic. So
it was a victory for realism, at least, when MTV decided to supplement its hit
reality shows “16 and Pregnant” and “Teen Mom” with last week’s special, “No
Easy Decision,” which followed Markai Durham, a teen mother who got pregnant a
second time and chose abortion.
MTV being MTV, the special’s attitude was resolutely pro-choice. But it was a
heartbreaking spectacle, whatever your perspective. Durham and her boyfriend are
the kind of young people our culture sets adrift — working-class and
undereducated, with weak support networks, few authority figures, and no script
for sexual maturity beyond the easily neglected admonition to always use a
condom. Their televised agony was a case study in how abortion can
simultaneously seem like a moral wrong and the only possible solution — because
it promised to keep them out of poverty, and to let them give their first
daughter opportunities they never had.
The show was particularly wrenching, though, when juxtaposed with two recent
dispatches from the world of midlife, upper-middle-class infertility. Last month
there was Vanessa Grigoriadis’s provocative New York Magazine story “Waking Up
From the Pill,” which suggested that a lifetime on chemical birth control has
encouraged women “to forget about the biological realities of being female ...
inadvertently, indirectly, infertility has become the Pill’s primary side
effect.” Then on Sunday, The Times Magazine provided a more intimate look at the
same issue, in which a midlife parent, the journalist Melanie Thernstrom,
chronicled what it took to bring her children into the world: six failed in
vitro cycles, an egg donor and two surrogate mothers, and an untold fortune in
expenses.
In every era, there’s been a tragic contrast between the burden of unwanted
pregnancies and the burden of infertility. But this gap used to be bridged by
adoption far more frequently than it is today. Prior to 1973, 20 percent of
births to white, unmarried women (and 9 percent of unwed births over all) led to
an adoption. Today, just 1 percent of babies born to unwed mothers are adopted,
and would-be adoptive parents face a waiting list that has lengthened beyond
reason.
Some of this shift reflects the growing acceptance of single parenting. But some
of it reflects the impact of Roe v. Wade. Since 1973, countless lives that might
have been welcomed into families like Thernstrom’s — which looked into adoption,
and gave it up as hopeless — have been cut short in utero instead.
And lives are what they are. On the MTV special, the people around Durham
swaddle abortion in euphemism. The being inside her is just “pregnancy tissue.”
After the abortion, she recalls being warned not to humanize it: “If you think
of it like [a person], you’re going to make yourself depressed.” Instead, “think
of it as what it is: nothing but a little ball of cells.”
It’s left to Durham herself to cut through the evasion. Sitting with her
boyfriend afterward, she begins to cry when he calls the embryo a “thing.”
Gesturing to their infant daughter, she says, “A ‘thing’ can turn out like that.
That’s what I remember ... ‘Nothing but a bunch of cells’ can be her.”
When we want to know this, we know this. Last week’s New Yorker carried a poem
by Kevin Young about expectant parents, early in pregnancy, probing the mother’s
womb for a heartbeat:
The doctor trying again to find you, fragile,
fern, snowflake. Nothing.
After, my wife will say, in fear,
impatient, she went beyond her body,
this tiny room, into the ether—
... And there
it is: faint, an echo, faster and further
away than mother’s, all beat box
and fuzzy feedback. ...
This is the paradox of America’s unborn. No life is so desperately sought after,
so hungrily desired, so carefully nurtured. And yet no life is so legally
unprotected, and so frequently destroyed.
The Unborn Paradox, NYT, 2.1.2011,
http://www.nytimes.com/2011/01/03/opinion/03douthat.html
U.S.
Alters Rule on Paying for End-of-Life Planning
January 4,
2011
The New York Times
By ROBERT PEAR
WASHINGTON
— The Obama administration, reversing course, will revise a Medicare regulation
to delete references to end-of-life planning as part of the annual physical
examinations covered under the new health care law, administration officials
said Tuesday.
The move is an abrupt shift, coming just days after the new policy took effect
on Jan. 1.
Many doctors and providers of hospice care had praised the regulation, which
listed “advance care planning” as one of the services that could be offered in
the “annual wellness visit” for Medicare beneficiaries.
While administration officials cited procedural reasons for changing the rule,
it was clear that political concerns were also a factor. The renewed debate over
advance care planning threatened to become a distraction to administration
officials who were gearing up to defend the health law against attack by the new
Republican majority in the House.
Although the health care bill signed into law in March did not mention
end-of-life planning, the topic was included in a huge Medicare regulation
setting payment rates for thousands of physician services. The final regulation
was published in the Federal Register in late November. The proposed rule,
published for public comment in July, did not include advance care planning.
An administration official, authorized by the White House to explain the mix-up,
said Tuesday, “We realize that this should have been included in the proposed
rule, so more people could have commented on it specifically.”
“We will amend the regulation to take out voluntary advance care planning,” the
official said. “This should not affect beneficiaries’ ability to have these
voluntary conversations with their doctors.”
The November regulation was issued by Dr. Donald M. Berwick, administrator of
the Centers for Medicare and Medicaid Services and a longtime advocate for
better end-of-life care. White House officials who work on health care
apparently did not focus on the part of the rule that dealt with advance care
planning.
The decision to drop the reference to end-of-life care upset some officials at
the Department of Health and Human Services, who said the administration ought
to promote discussions of such care. Such discussions help ensure that patients
get the care they want, the officials said.
During debate on the legislation, Democrats dropped a somewhat similar proposal
to encourage end-of-life planning after it touched off a political storm.
Republicans said inaccurately that the House version of the bill allowed a
government panel to make decisions about end-of-life care for people on
Medicare.
Sarah Palin, the 2008 Republican vice-presidential candidate, said in the summer
of 2009 that “Obama’s death panel” would decide who was worthy of health care.
Representative John A. Boehner of Ohio, the House Republican leader who is to
become speaker on Wednesday, said the provision could be a step “down a
treacherous path toward government-encouraged euthanasia.”
The health care bill passed by the House in 2009 allowed Medicare to pay doctors
for discussions of end-of-life care, including advance directives, in which
patients can indicate whether they want to forgo or receive aggressive
life-sustaining treatment.
The provision for advance care planning was not included in the final health
care overhaul signed into law by President Obama. Health policy experts assumed
that the proposal had been set aside — until a similar idea showed up in the
final Medicare regulation in November.
U.S. Alters Rule on Paying for End-of-Life Planning, NYT,
4.1.2011,
http://www.nytimes.com/2011/01/05/health/policy/05health.html
|